

INTRODUCTION
Dentistry is all about little details. One of those details that can cause clinical frustration is the removal of excess cement around a dental restoration. The negative effects of residual cement around implant crowns have been well documented and include periodontal inflammation, swelling, soreness, increased probing depths, bleeding or exudation upon probing, and radiographic bone loss.1 Aside from the negative effects of leaving excess cement at the gingival margin, excess cement in the interproximal area must be removed in order to allow patients to floss easily. Cement cleanup is often more difficult with resin cements. According to a Practice-Based Research Network study, almost 40% of single-unit crowns in the United States are bonded with resin cement.2 Therefore, cleaning resin cement is an important clinical procedure that is routinely performed in US dental offices. The methods to accomplish this clinical step, however, are rarely discussed. This article will focus on a new type of dental floss that has the strength and shred resistance necessary to clean residual resin cement effectively. Additionally, several other methods for excess cement removal will be discussed.
Perhaps the easiest and most cost-effective method to clean excess residual cement is using dental floss. Dental floss is available in several varieties (Figure 1).
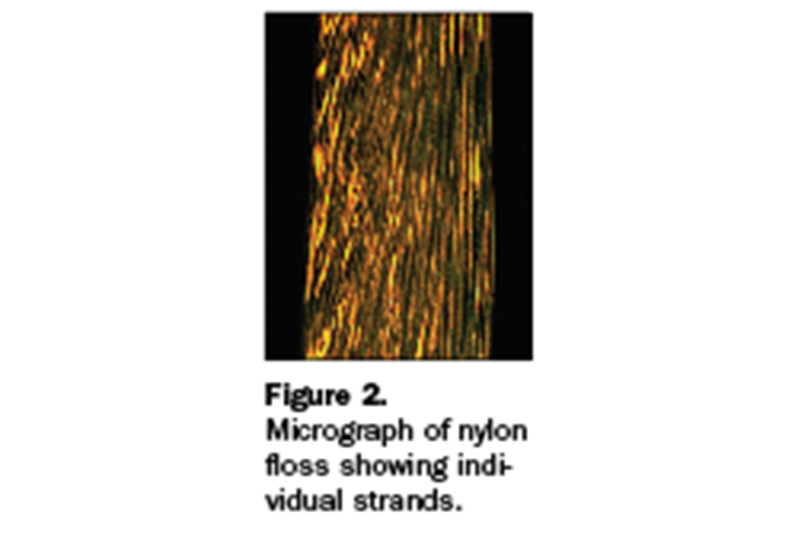
The most common type of dental floss is nylon floss. Nylon floss is composed of many thin nylon fibers (Figure 2), and it can be waxed or unwaxed. Waxed floss allows the floss to glide between teeth and helps to prevent shredding. Nylon floss is also offered in a thicker version, which is sometimes called floss tape. Floss tape contains more strands of nylon fibers, and it is stronger than regular nylon tape. Therefore, floss tape can be used to remove more tenacious pieces of residual cement. The thickness of floss tape, however, will limit its ability to slide between tight contacts. The major disadvantage of all nylon floss is that it will shred during use due to the tearing of individual nylon fibers. Shredded floss is not only ineffective but will also leave remnants of small nylon fibers that must later be identified and removed.
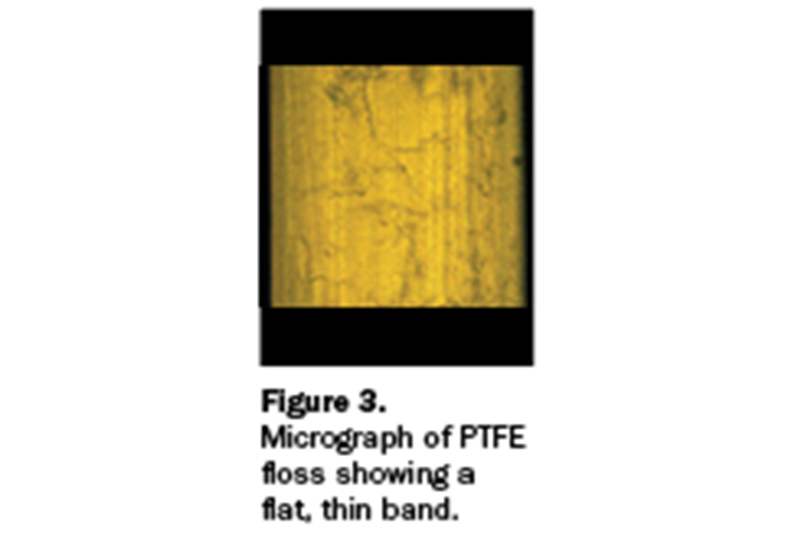
Another type of floss is polytetrafluoroethylene (PTFE) floss. PTFE is also referred to as Teflon. PTFE floss is composed of a thin band of material (Figure 3). The thinness and flexibility of PTFE floss allows it to glide between tight contacts. A clinical trial reported that PTFE floss required less force than nylon floss to pass through interproximal contacts.3 Another clinical trial reported that 75% of participants preferred flossing with PTFE floss rather than waxed nylon floss.4 Some PTFE floss is covered with a coating to give the floss texture to help remove plaque. This coating can shred between teeth, causing the patient to feel a tight contact. The major disadvantage of PTFE floss, however, is that it is generally weaker than nylon floss. When flossing very tight contacts or removing hard pieces of cured excess cement, PTFE floss may snap.
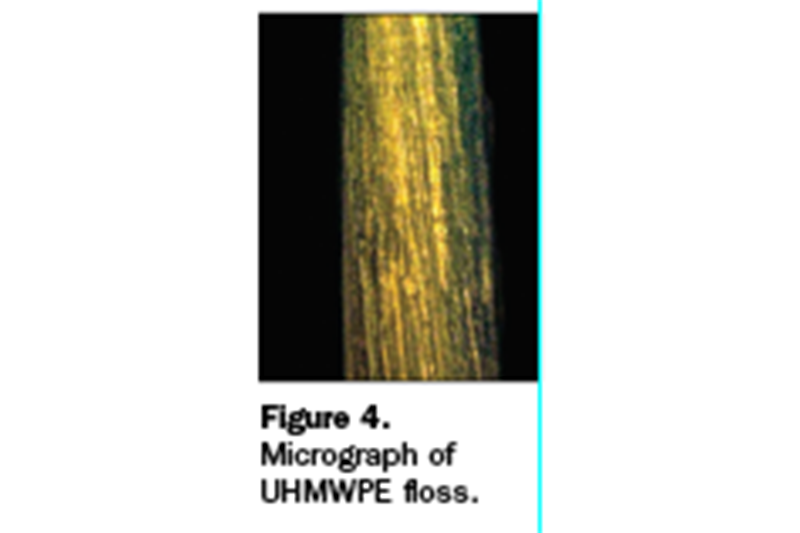
A new type of dental floss is available that is formulated with ultra-high molecular-weight polyethylene (UHMWPE). The brand name of this floss is Gorilla Floss (Piksters). This floss is stronger than nylon floss tape, thin or thinner than waxed nylon floss, and shred-resistant (Figure 4). This floss is ideal for separating tight contacts and removing excess cement.
The strength and modulus (flexibility) of several different types of dental floss were compared using a universal testing machine. A piece of floss was tied to the base of the machine, and the other end was connected to a force sensor. The floss was then pulled apart in tension at 10 mm/min until the floss snapped. The force per extension of a representative sample of several types of floss is presented in Figure 5. The peak force is the required amount of force to snap the floss. The slope of the line represents the flexibility of the floss (the higher slope is stiffer, and the lower slope is more flexible). The UHMWPE floss was more than twice as strong as floss tape and over 5 times as strong as PTFE tape. The strength of this floss will prevent it from snapping when cleaning cement from tight contacts. Additionally, Figure 5 demonstrates that PTFE floss is more flexible than nylon floss.

The thicknesses of different types of floss were evaluated by measuring them with image analysis software in a digital light microscope. Representative sections of floss are presented in Figure 6. Although PTFE tape is wide, it is also very thin, allowing it to slide into tight contacts more easily. The UHMWPE floss is slightly thinner than waxed nylon floss. The thinness of the floss should improve its ability to slide between contacts.
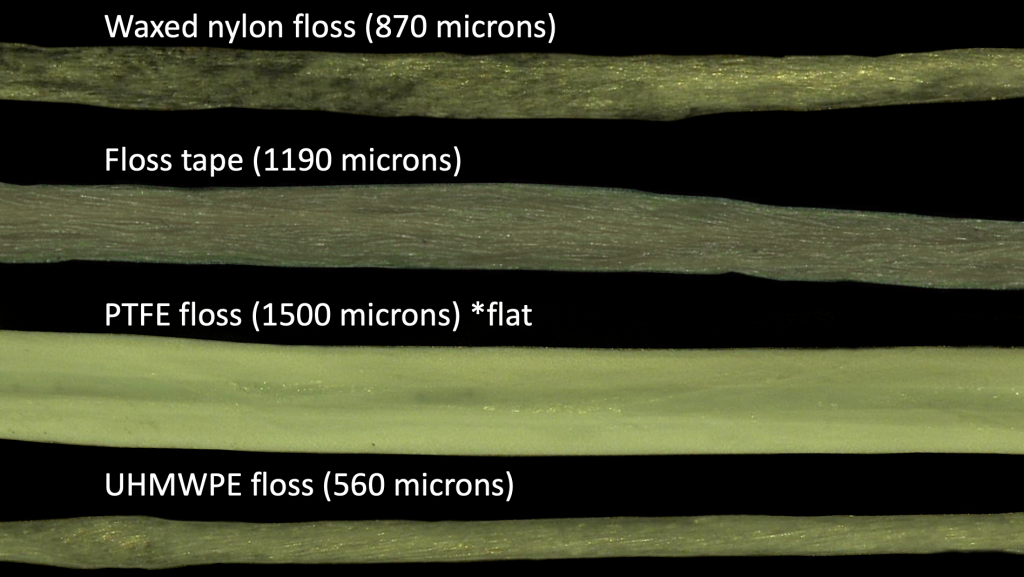
Figure 6. Thickness of different types of floss (top to bottom): waxed nylon floss, floss tape, PTFE floss, and UHMWPE floss.
CASE REPORT
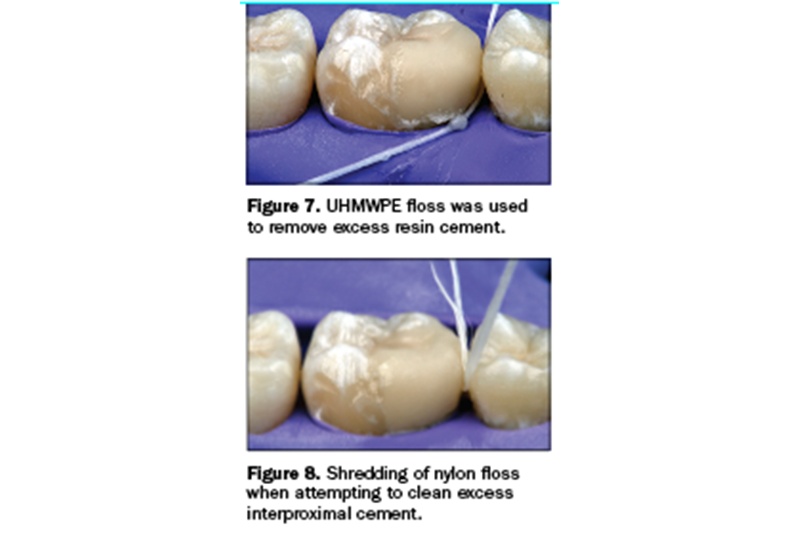
UHMWPE floss was used to clean excess resin cement at the margin of an indirect resin composite onlay (Figure 7). A knot was tied in the floss to help grip the cement. The UHMWPE floss was able to pass through the interproximal contact without shredding or snapping. For comparison, a piece of waxed nylon floss was inserted between the teeth to remove excess cement, and shredding occurred when an attempt was made to remove the floss (Figure 8). Strands of the shredded floss required removal with additional floss.
DISCUSSION
UHMWPE floss is a strong, shred-resistant, relatively thin floss that is ideal for both separating teeth with tight contacts and removing excess cured cement. It is a fast and inexpensive first choice for the removal of excess cement. Additionally, it is safe on the patient’s soft tissue, and it’s a familiar tool for the patient that should not cause much dental anxiety. Another advantage of UHMWPE floss is that it is firm enough to be threaded through gingival embrasures without the need for a floss threader.
Occasionally, however, there are pieces of tenacious resin cement or very tight contacts that require additional tools. One method of separating a tight contact is to physically separate the teeth such that the bond between the teeth is broken. One way to do this is to insert a wedge firmly between the teeth. Tooth separations of 90 to 150 μm have been recorded following 1 minute of wedging with a wooden wedge.5 Another method is to place a flat metal dental instrument into the occlusal embrasure between the teeth and gently twist it.
Another method to break a tight contact is to force a metal band between the teeth. Occasionally, a flat Tofflemire matrix band may be inserted between the teeth. Metal saws can also be used to separate a contact; however, caution should be taken to prevent opening the contact with the saw. Alternatively, the separation of teeth may be aided by removing excess cement in the occlusal or gingival embrasure. Excess cement may be removed from the occlusal embrasure with a #12 blade. Excess cement in the gingival embrasure can sometimes be removed with a metal explorer tip or a floss threader.
Finally, excess cement cleanup can be greatly simplified by preventing the bonding of adjacent teeth and minimizing excess cement. Teflon tape can be stretched on neighboring teeth to prevent resin cement from bonding to adjacent teeth. Wiping excess uncured cement with a microbrush and then cleaning the remaining cement after tack curing can help prevent the difficulties of cleaning fully cured cement.
REFERENCES
1. Pauletto N, Lahiffe BJ, Walton JN. Complications associated with excess cement around crowns on osseointegrated implants: a clinical report. Int J Oral Maxillofac Implants. 1999;14(6):865–8.
2. Lawson NC, Litaker MS, Ferracane JL, et al; National Dental Practice-Based Research Network Collaborative Group. Choice of cement for single-unit crowns: Findings from The National Dental Practice-Based Research Network. J Am Dent Assoc. 2019;150(6):522-530. doi:10.1016/j.adaj.2019.01.021
3. Dörfer CE, Wündrich D, Staehle HJ, et al. Gliding capacity of different dental flosses. J Periodontol. 2001;72(5):672–8. doi:10.1902/jop.2001.72.5.672
4. Ciancio SG, Shibly O, Farber GA. Clinical evaluation of the effect of two types of dental floss on plaque and gingival health. Clin Prev Dent. 1992;14(3):14–8.
5. Hellie CM, Charbeneau GT, Craig RG, et al. Quantitative evaluation of proximal tooth movement effected by wedging: a pilot study. J Prosthet Dent. 1985;53(3):335-341. doi:10.1016/0022-3913(85)90505-0
ABOUT THE AUTHORS
Dr. Lawson is the director of the division of biomaterials and program director of the biomaterials residency program at the University of Alabama at Birmingham (UAB) School of Dentistry. He can be reached at nlawson@uab.edu.
Dr. Mangla is a second-year resident in the biomaterials program at UAB.
Dr. Mantri is a first-year resident in the biomaterials program at UAB.
Disclosure: The authors report no disclosures.