

Dr. Esther Feldman ponders what came first, the open bite or the habit?
Which came first, the chicken or the egg?
Open bites are one of the most difficult classes of malocclusions that orthodontists are faced with in practice. That’s because the success of their resolution is entirely dependent on correctly addressing the etiology. The root cause can be skeletal, which most often requires surgical intervention; it can be dental or a combination of the two. Open bites develop as a result of the interaction of many different etiologic factors, including thumb- and finger-sucking, tongue habits, airway obstruction, and true skeletal growth abnormalities. All anterior open bites present with an accompanying tongue thrust to prevent drooling upon swallowing. It’s not always obvious to determine which came first — the open bite or the habit. Vertical growth is the last dimension to be completed, asnd therefore, treatment may appear to be successful at one point and fail later, in spite of good retention. In the case of relapse, these cases tend to seek retreatment in adulthood.
Diagnosis and plan
Paul, a 30-year old male, presented to my office last March. He had noticed his bite getting progressively worse and was frustrated that he was unable to bite into a slice of pizza. He had no significant medical history and had been treated by an orthodontist in his early teenage years. Skeletally, Paul presented as a Class I, and his anterior open bite was determined to be of dental origin. This relapse case had a problem list that included a 4 mm anterior open bite, a Bolton discrepancy (upper lateral incisors were deficient), mild crowding in both arches, mild overjet of 2.5 mm, and a mild Class II malocclusion on both sides. The lower midline deviated 1 mm to the right, and a tongue thrust was observed. We discussed treatment options, and the patient desired clear aligners with high- frequency vibration (HFV) for acceleration, comfort, and increased predictability. Like most young professionals, Paul wanted the outcome to be achieved as quickly and predictably as possible. In order to meet these objectives, he was aware of the number of attachments needed to help with the bite-closing mechanics and the placement of elastics. We discussed utilizing buccal and palatal attachments on the upper anteriors to help discourage his tongue habit. Finally, Paul was not concerned with his small lateral incisors and rejected the possibility to build them up. He instead opted for lower interproximal reduction (IPR) to help manage his tooth size discrepancy.
Figure 1
The catalyst: HFV
In the case of anterior open bite and aligners, the anterior teeth do not get seated into the aligners by the force of occlusion. Therefore, it’s imperative to use adjunctive measures to obtain some vertical force to help properly seat the aligners on these teeth. The VPro™ high-frequency vibration (HFV) device from Propel Orthodontics is my go-to solution to increase predictability and reduce pain. It is both efficient and effective, while simultaneously soothing to the patient’s tender dentition due to the increased blood flow in the mouth.
For this case, I instructed the patient to bite down on the VPro for 5 minutes to achieve full mouth seating, as well as an additional 5 minutes isolating it to each anterior tooth. We also discussed rotating the device, if necessary, so that the high frequency vibrational force could engage every single tooth and cause the catabolic reaction of recruiting cytokines and activation of periodontal ligament cells to assist with bone remodeling.1 In order to achieve his treatment objectives, the emphasis was placed on compliance, both with the VPro and his aligner wear. As a result of using the VPro, which served as the biological and physical catalyst, Paul was able to progress on a 5-7 day aligner change interval. The VPro also made it possible to reduce office visits, as we delivered more aligners to swap through between visits.
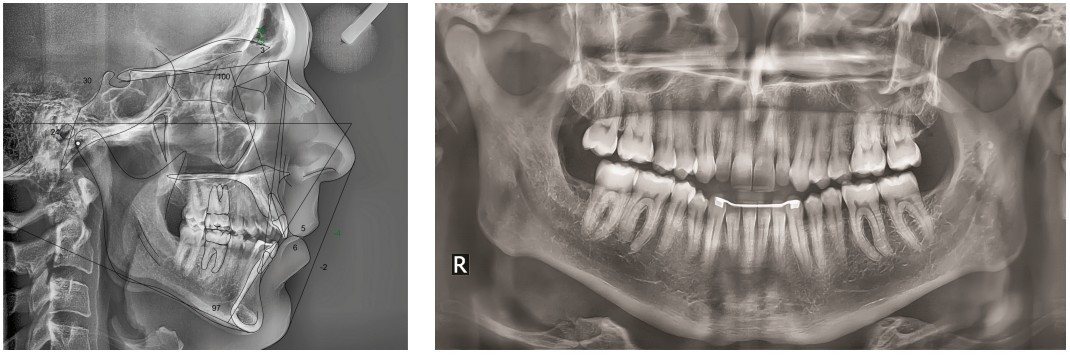
Figure 2 (left), Figure 3 (right)
Results
We reached our goal of closing Paul’s anterior open bite and correcting the mild Class II in eight total visits, including refinements. A treatment, which normally would have taken 12 to 18 months and several more visits, was completed to the highest clinical standards in a quick 9 months. This was a direct result of excellent patient compliance in conjunction with HFV. The use of HFV allowed for fewer office visits, reduced chair time, and a seamless treatment experience. The VPro was key to engaging his maxillary anterior teeth into the aligners and keeping his case tracking accordingly. Paul is retained with Vivera® (Invisalign®) retainers. He still uses his VPro in retention to take advantage of the anabolic effects of HFV. When used without orthodontic force, HFV helps to increase bone density1 while maintaining the correct fit of the retainers over his teeth.
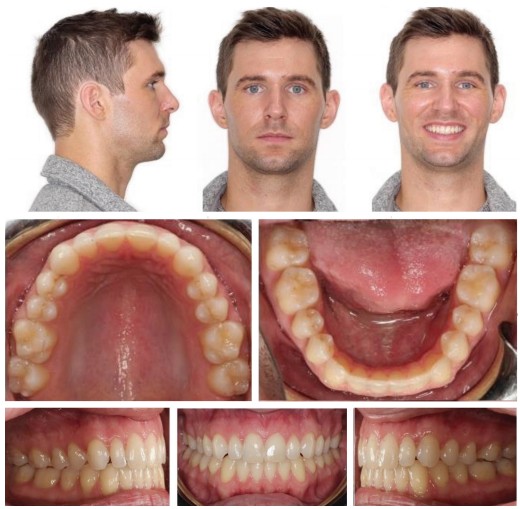
Figure 4
Conclusion
The success of treating an anterior open bite with aligners is dependent on patient compliance and the correct fit of the aligners over the teeth. To achieve this, adjuncts to treatment, particularly HFV devices such as the VPro, are necessary to keep the case on track and to achieve treatment goals in a predictable and timely manner. Now more than ever, reducing patient visits is of the utmost importance. VPro affords me the confidence to see patients less and deliver more aligners between visits. Concerning retention, we know that all cases have a chance of relapse, especially open-bite cases. VPro is used for all my cases in retention — if the case goes off track at all, the patient uses the VPro to vibrate the case back into place.