

The American Academy of Implant Dentistry estimates that 3 million Americans have dental implants to replace missing teeth. Another 400,000 implants are placed each year. As the dental implant industry continues to grow in popularity, control and precision before and during implant surgery, including planning and placement, are essential. As technologies advance, digital dentistry through CBCT scanning is certainly becoming the standard of care. There is a new kid on the block that elevates precision implant placement to a new level. It is called dynamic navigation (DN), and it is a dynamic computer-aided system that allows the clinician real-time visualization of the virtual plan as the drill is in motion. This article explicitly addresses the X-Guide Dynamic 3D System (X-Nav Technologies) that provides this turn-by-turn guidance during live surgery. It’s as easy as 1, 2, 3.
Whether you are currently placing implants free-handed or using a surgical guide, there is certainly a level of inaccuracy built into both of these methods. Freehand (FH) implant placement breeds inaccuracy as the surgeon creates the osteotomy using adjacent and opposing teeth as positioning guides.1-3 A custom-fabricated surgical guide (a static navigation [SN]), although more accurate, has some degree of play built into the system. Success may be limited by CBCT discrepancies and incorrect placement or instability of the guide. There is definitely more accuracy in tooth-supported guides than in bone- or mucosal-supported ones.4 When mucosal-borne, there is a standard deviation (SD) for angulation of the implant of 2.71° as compared to an SD of 9.92° when freehand.3 A surgical guide requires an additional appointment and lab costs as well as intraoral access of all components at the time of surgery. Using a surgical guide, the position of the implant is not alterable during surgery unless the guide is abandoned and FH positioning is used.3 Similar studies have been completed, which also have taken into consideration the platform and apical deviation of positioning. Most notably, the platform deviation for FH placement showed 1.78 +/- 0.77 mm for implant platform and 2.27 +/- 1.02 mm for apical positioning. The DN outperforms the SN by providing approximately 0.5 mm more accuracy on average in angulation of implant placement and 0.15 mm in platform deviation and 0.23 mm in apical positioning precision.1 Enhanced accuracy decreases the practitioner’s stress and elevates his or her practice’s impression, all while making the surgery visible. This DN system offers precision in one appointment without additional lab fees. Although the SD for DN-placed implants has been found to be similar to that of extremely accurate surgical guides,5 for the above-mentioned reasons, DN is more desirable. The drawbacks to the use of DN technology are few. Of course, there is a cost and a learning curve to the system. In addition, few studies discuss the surgical experience of the practitioner with implant placement in general, which should also be considered when assessing implant placement speed, accuracy, and success rates.6 Studies report the learning curve to be completed by the 20th surgery.1 The following case report will discuss the ease of use, precision accuracy, stress reduction, and sophistication of the X-Guide system.
CASE REPORT
It’s as simple as 1, 2, 3 after choosing your case for implant placement:
1. CBCT SCAN with fiducials
2. Digital treatment planning
3. Calibration and dynamic navigation
CBCT SCAN With Fiducials
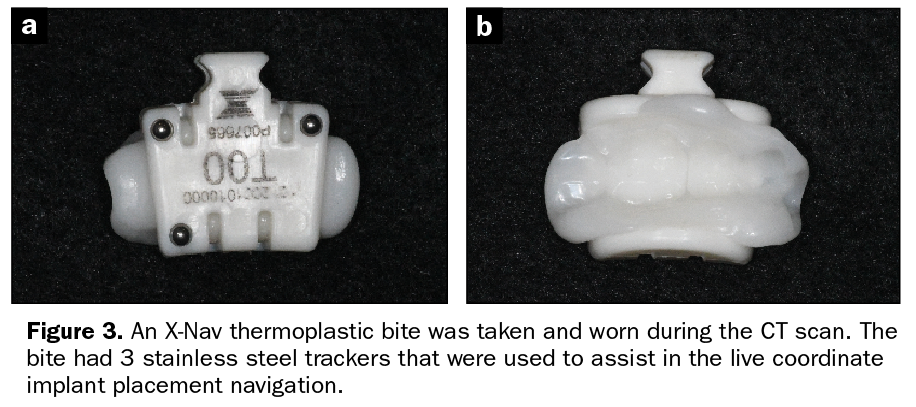
Our patient presented after 4 months of healing following extraction and bone grafting in the lower left first molar region (Figure 1). A digital intraoral scan of the mouth was obtained (Figure 2). Whether doing same-day surgery or not, the next step includes an innovative bite to be taken using the X-Clip. This X-Clip is a resin bite block lined with a thermoplastic liner that is heated in a water bath to soften it (Figure 3). The X-Clip is then placed in the contralateral side of the implant placement, firmly covering 2 to 3 teeth for 15 seconds. Immediately remove the X-Clip from the mouth and place it in an ice bath for 20 seconds. Reinsert it in the mouth to confirm a solid fit without rock (this step is critical for accurate surgery).
Figure 1. A preoperative lateral view of a 60-year-old’s left mandible prior to implant placement.
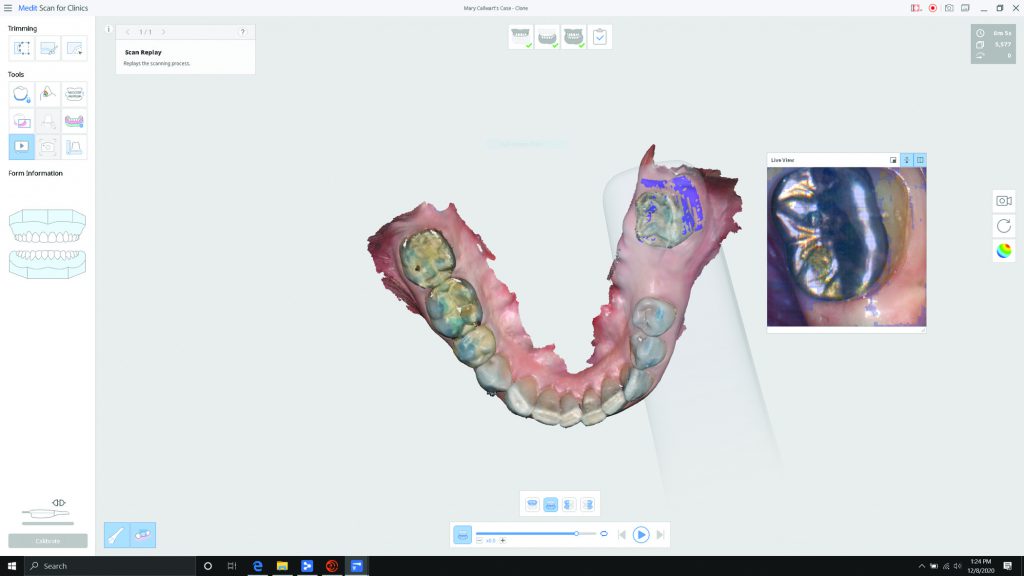
Figure 2. An i700 (Medit) intraoral scan was taken for precision digital treatment planning.
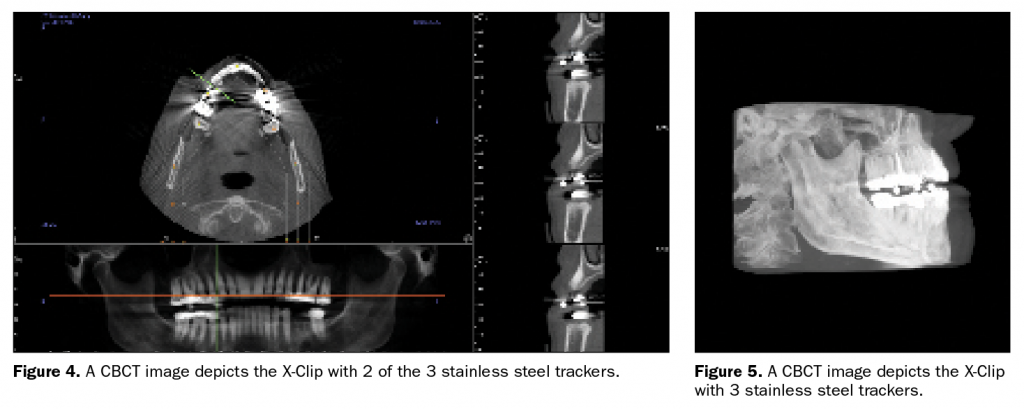
For this reason, the X-Clip should not be placed on provisionals or loose teeth unless the primary stability of the clip is achievable. Embedded in the X-Clip are 3 stainless steel trackers, which function as fiducial markers to translate 3 virtual points on the CBCT scan (Figures 4 and 5). The X-Nav technology allows the 3 virtual trackers to merge with the same 3 live trackers to assist in facilitating the surgeon’s digital treatment plan in 3D visualization at the time of surgery. These 3 markers must be rigid and predictably reproduced for accurate results. Place the X-Clip on the patient and take a CBCT scan of the mouth. A bilateral scan is needed to capture the entire X-Clip and implant placement location.
The X-Guide allows the surgeon to navigate with precise movements of the handpiece in all 3 planes of space for millimeter-by-millimeter accuracy. When all 3 fiducials have green indicators, the system calibration is within 200 μm.7 This technology can be delivered the same day, which saves time, energy, and money. This DN is used in many specialties, such as general surgery, neurosurgery, and oncology, with increased accuracy and precision.
Digital Treatment Planning
Using appropriate treatment planning software (DTX Studio [Nobel Biocare] was used in this case), and ideally, a restoratively driven mindset, can and should be done only from the crown down, based on prosthetic needs, but also with consideration for the opposing arch for a proper occlusal load. With the advent of angulated screw channel design, ideal implant placement, as well as ideal prosthetics, are obtainable. Intraoral scanning can also be merged at this time for more precision (Figure 6). From the digital plan, provisionalization can be treatment planned and fabricated for placement at the time of surgery, if desired (Figure 7).

Figure 6. An intraoral scan from the i700 was merged with the CT scan and DTX Studio software (Nobel Biocare) to treatment plan from the top down. Ideal tooth placement was generated first, with implant placement following later.

Figure 7. From the digital treatment plan, a model and winged provisional were printed.
Calibration and Dynamic Navigation
Whether completing same-day surgery or not, calibration of the X-Nav instrumentation should occur prior to seating your patient. Proprietary trackers, which are similar to barcodes, attach to the surgical handpiece and the X-Clip. Calibrating the 2 allows the system to have real-time guidance in 3 dimensions. When using the handpiece, active rays are emitted from a light source and a tracking camera overhead. The drill tip is the third point tracked that is calibrated on a plate that is also barcoded (Figure 8).
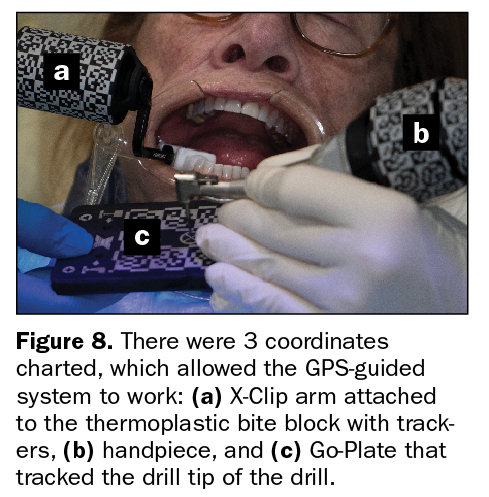
Once the patient is seated, the X-Clip with the Patient Tracker is snapped onto the teeth in the contralateral arch during implant surgery. Touching the drill tip to the Go-Plate calibrates the drill. By touching an adjacent tooth visible on the screen, the accuracy of the system’s position is confirmed. The camera identified the patterns at all 3 coordinates: the surgical handpiece, the X-Clip arm, and the tip of the drill. The barcodes on the surgical handpiece, the X-Clip arm, and the Go-Plate must be in view of the camera for the system to “go live.” These 3 calibration tools are rechecked between each drill and implant to confirm accuracy in the system.
DN Implant Placement
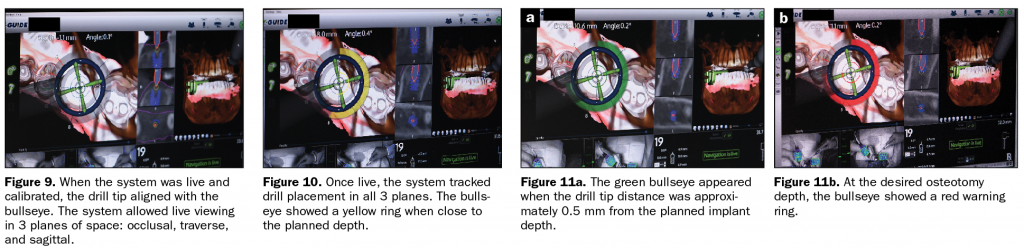
Once the above steps are complete, live navigation surgery begins. Following the bullseye makes precision surgery simple (Figure 9). The bullseye tracks live in 3 dimensions and is visible simultaneously in all 3 dimensions on the screen. The bullseye ring changes color from blue to yellow when the desired osteotomy depth is nearly complete (Figure 10). This GPS-like guided system increases the confidence of the dentist and certainly the patient. The bullseye turns to green when within 0.5 mm of the desired length (Figure 11), then to red, indicating osteotomy depth is achieved (Figure 12). As previously mentioned, maintaining a precise perpendicular angle to the blue crosshairs on the bullseye can achieve precision within 200 μm of the treatment plan. Multiple views are displayed simultaneously for the clinician to monitor the osteotomy depth and drill angle in all planes in order to control every movement with pinpoint accuracy.7 Once the proper width and length of the osteotomy are obtained, the same system check steps and live navigation occurs for implant placement (Figure 13). Hand torque confirmation is the final step in implant placement, followed by provisionalization. This case was torqued to 35 Ncm (Figure 14). During the surgical procedure, the surgeon follows the screen while the assistant verifies the intraoral positioning.
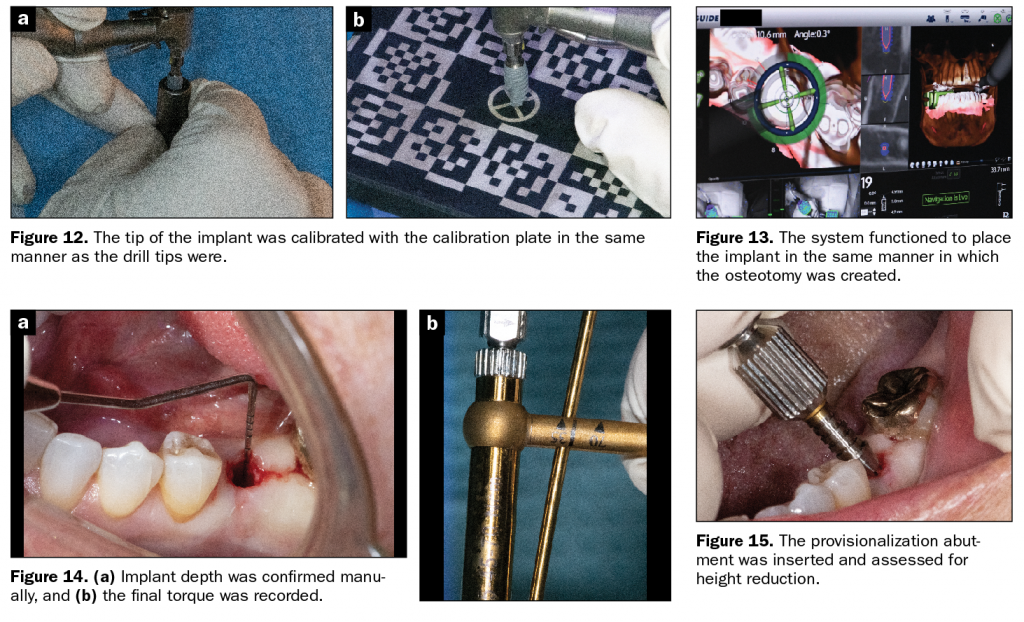
This patient was desirous of immediate provisionals. A provisionalization abutment was inserted and assessed for height reduction (Figure 15). The abutment was reduced as needed and manually screwed into place (Figure 16). The provisional was tried into the mouth to ensure appropriate abutment height, and the provisional shell was relined with resin. The author fabricated the provisional with wings to double-check for complete and accurate seating of the provisional (Figure 17). The provisional and abutment were removed from the mouth once the resin reline completely set. Wings were then removed, and access was made through the occlusal from the apical base of the temporary abutment with the access drill provided. The margins were filled in with flowable resin, contoured, and polished to sculpt the tissue during the healing phase as desired (Figure 18).
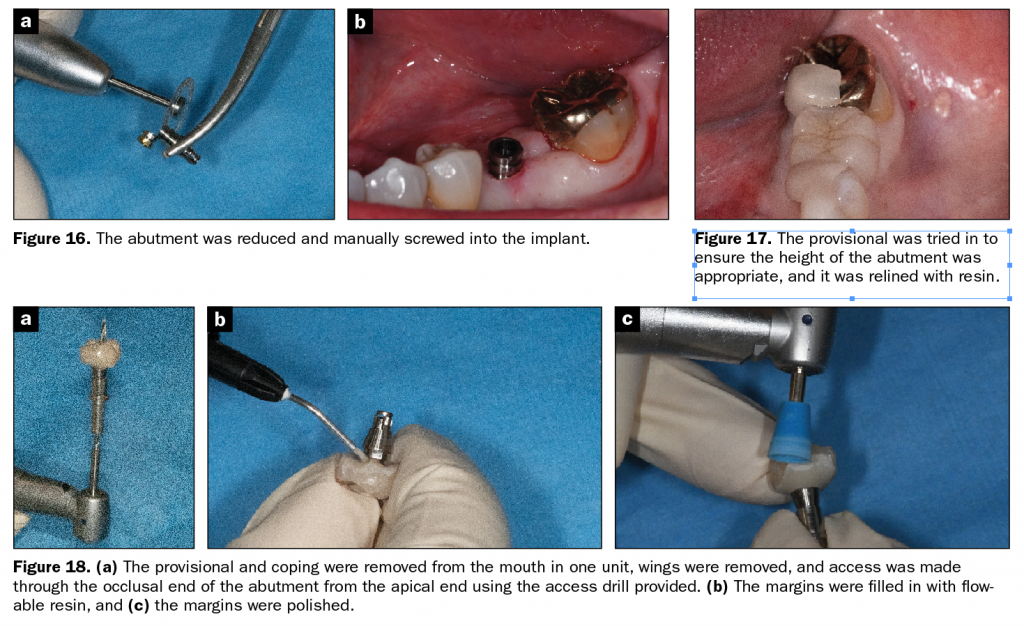
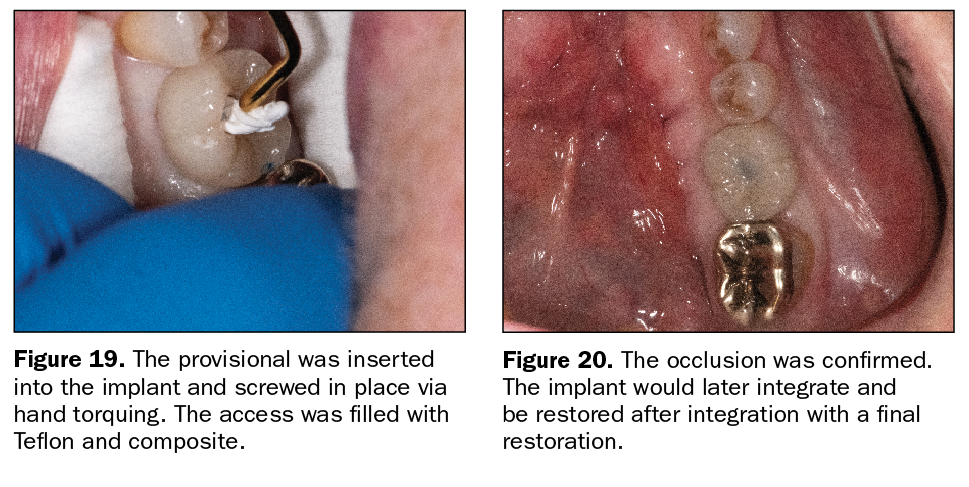
The provisional was then luted to the temporary abutment, inserted into the implant, and screwed in place via hand torquing. The access was filled with Teflon and composite (Figure 19). The provisional was left out of occlusion and confirmed with articulating paper and shim stock.
The implant would then integrate and be restored in approximately 4 months with a final restoration (Figure 20).
IN SUMMARY
Recently, advances in implant dentistry have created a greater degree of accuracy through new technology. A shift is occurring from the FH placement of implants and traditional use of surgical guides to more precision with DN implant placement. The X-Nav technology can be easily implemented with current CT scanners and can offer same-day implant placement with precision up to 200 μm. Changes to the plan can be made during the surgical procedure. Live visualization of the oral field is achieved for implant position, angle, and depth at every turn of the handpiece, which offers step-by-step control. DN is as easy as 1, 2, 3, saving the practitioner time, energy, and money while increasing precision and peace of mind in the field of dental implant placement. In the future, robots may be the ones placing the implants!8
References
1. Block MS, Emery RW, Lank K, et al. Implant placement accuracy using dynamic navigation. Int J Oral Maxillofac Implants. 2017;32(1):92-99. doi:10.11607/jomi.5004
2. Block MS, Emery RW, Cullum DR, et al. Implant placement is more accurate using dynamic navigation. J Oral Maxillofac Surg. 2017l;75(7):1377-1386. doi:10.1016/j.joms.2017.02.026
3. Block MS, Emery RW. Static or dynamic navigation for implant placement–choosing the method of guidance. J Oral Maxillofac Surg. 2016;74(2):269-77. doi:10.1016/j.joms.2015.09.022
4. Ozan O, Turkyilmaz I, Ersoy AE, et al. Clinical accuracy of 3 different types of computed tomography-derived stereolithographic surgical guides in implant placement. J Oral Maxillofac Surg. 2009;67(2):394-401. doi:10.1016/j.joms.2008.09.033
5. Emery RW, Merritt SA, Lank K, et al. Accuracy of dynamic navigation for dental implant placement-model-based evaluation. J Oral Implantol. 2016;42(5):399-405. doi:10.1563/aaid-joi-D-16-00025
6. Pellegrino G, Bellini P, Cavallini PF, et al. Dynamic navigation in dental implantology: the influence of surgical experience on implant placement accuracy and operating time. An in vitro study. Int J Environ Res Public Health. 2020;17(6):2153. doi:10.3390/ijerph17062153
7. Panchal N, Mahmood L, Retana A, et al. Dynamic Navigation for Dental Implant Surgery. Oral Maxillofac Surg Clin North Am. 2019;31(4):539-547. doi:10.1016/j.coms.2019.08.001
8. Cheng KJ, Kan TS, Liu YF, et al. Accuracy of dental implant surgery with robotic position feedback and registration algorithm: An in-vitro study. Comput Biol Med. 2021;129:104153. doi:10.1016/j.compbiomed.2020.104153
ABOUT THE AUTHOR
Dr. Stonisch is a pioneer in dentistry with more than 2,000 continuing education credit hours earned and 3.5 decades of experience. Accredited by the American Academy of Cosmetic Dentistry, a distinction held by fewer than approximately 40 female dentists worldwide, Dr. Stonisch combines her experience with degrees in art and chemistry to produce smart, sophisticated smiles in her comprehensive dental practice in Grosse Pointe, Mich. She is a Diplomate in the International Congress of Oral Implantologists and a mentor at the Kois Center in Seattle. Dr. Stonisch was the 2017 recipient of the Excellence in Business Award given by her community. She was also the recipient of the 2018 Spiritus Award from her alma mater, the University of Detroit Mercy School of Dentistry. Dr. Stonisch has authored an easy-to-read, step-by-step guide to oral health and common dental dilemmas for consumers (patients) called Smile Fit, along with a companion workbook, Smile Fitness. She holds 3 patents for her SMILE-NOW peel-and-stick dental templates, which allow dentists as well as patients to quickly and easily see smile possibilities. She can be reached at thesmileartist@comcast.net.
Disclosure: Dr. Stonisch reports no disclosures.