

INTRODUCTION
Implant dentistry has become a prominent treatment modality in many of our dental practices. Advances in engineering, design, and manufacturing have created fixtures that are both predictable, functional, and aesthetic. To become proficient in diagnosing and treatment planning, the practitioner must understand vital anatomy and the limitations to these popular modes of therapies. CBCT diagnosing allows visualization in 3 dimensions, maximizing implant placement to maximize the final restorative results.1,2 Modern implants are used to replace single teeth and multiple missing teeth and certainly aid in supporting partial or complete removable appliances. Full-arch, fixed prostheses require edentualism, or removal of non-restorable teeth. Candidacy for each of these potential implant patients is dictated by the quality and quantity of available bone and the individual’s overall health. Bone height and width are carefully considered. Proper and complete planning prior to any surgical intervention may improve the overall prognosis and meet patient satisfaction. CBCT scanning (PaX-i3D Green [Vatech America]) of the edentulous sites is done, and evaluations of vital anatomy, including nerve position and the sinuses, are made. Interocclusal spacing is measured. Interocclusal space per each arch is a critical review. With the All-on-X treatment modality, it is reported that 14 to 16 mm of available room is required for the final prosthesis per arch.3,4 This often indicates a significant reduction in bone height. Maintaining valuable hard tissue should be a consideration in any dental therapy as the bone morphology may change over time due to several physiologic conditions, including health, medication use, periodontal/peri-implant health, and maintenance.
Osteotomies for the Hahn Tapered Implant System (Glidewell) are completed through the surgical guides. In the case report in this article, these guides were fabricated by 3DDX (3D Diagnostix). CBCT DICOM files were electronically sent along with a cast of the maxillary and mandibular arches to create a 3D reconstruction of the patient’s CT scan. Virtual planning software revealed the vital anatomy and the ideal positioning of the implants in the available bone. Specific guided surgical drills compensate for the implant, soft tissue, and thickness of the guide itself. The body of this implant is tapered with a buttress thread pattern, allowing for initial stability and minimization of resorption in all bone types. The coronal microthreads aid in the preservation of crestal bone. The surface of the Hahn Tapered Implant System is a resorbable blast media to promote osseointegration. A machined collar facilitates soft-tissue maintenance, while its conical, internal hex connection provides a secure, stable prosthetic seal.5,6 Positioning of the implants is confirmed with conventional digital radiographs and a postoperative CBCT scan. Cover screws are threaded into the implants to allow for non-stressful, unerupted healing. After approximately 4 months of integration, the implants are uncovered, and prosthetic fabrication begins with an implant-level impression.
Although, with technology, visualizing implant position and the final prosthetic design becomes predictable, other factors need to be considered by the dentist. Bone anatomy and medical conditions are considered. Also, an often neglected part of this process is the desires of the patient. Meeting expectations helps in the overall satisfaction of any restoration. A tooth-up or tooth-down approach helps in diagnosing and explaining to the patient what the final prosthesis will be and how it will function. Bone loss is a natural, physiologic response to losing teeth.7 A major deterrent to the surgical placement of any implant by the dentist is the position of the mandibular nerve and the size of the maxillary sinuses. As root structure is removed, the maxillary sinuses collapse, and the hard tissue shrinks up and in the maxilla and down in the mandible.8 This compromises any ability for surgical placement. When a tooth root is removed, bone shrinkage physiologically occurs apically and palatally. Also, with the loss of support, the maxillary sinus will often collapse.
The limited bone availability may make implant placement challenging or unpredictable. Grafting procedures allow regeneration of bone at sites where deficiencies arise. Bone grafting techniques are an essential part of the implant dentist’s skill set. Autogenous grafts, or those harvested from another site in the patient’s mouth, may be the gold standard but require an invasive approach. Allograft materials, harvested from the bone of human donors, are popular since a secondary surgical site is not required. Cortico/cancellous particulates are processed to prevent disease transmission and antigenic responses.9-11
Internet searches by our patients are creating a high awareness of the benefits of our treatment. There are many options available to those who experience edentulism or decayed or periodontally involved teeth. Conventional dentures and partial dentures are at one end of the spectrum, while the “All-on-X” concept of removing all teeth with the result of fabrication of fixed, implant-retained prostheses with immediate or delayed loading is clearly on the other end of the process. Following proper diagnosing and treatment planning, implants can be considered to support dentition. Often, teeth may appear unaesthetic but are otherwise periodontally sound. The question that the dental professional must answer is whether removing teeth and viable bone structure to place dental implants along an edentulous arch and immediately loading them with a composite restoration that will eventually be replaced with a zirconia prosthesis is the best mode of therapy. Here, we will describe a circumstance in which the patient presented with missing teeth in the maxillary right and left posterior area and missing teeth in the mandible. The remaining dentition, although unaesthetic, was sound.
CASE REPORT
The patient presented in a severe Class III occlusal relationship and with a deep underbite (Figure 1). CBCT analysis demonstrated significant collapse of the right and left posterior sinuses and inadequate bone height and width to support dental implants (Figure 2). Because of the maxillary sinus collapse, in order to surgically place dental implants with a positive prognosis, the maxillary right and left sinuses were augmented using the Caldwel-Luc procedure, and the remaining maxillary dentition was temporized. The arch was opened, and the severe underbite was corrected to a more comfortable position for the patient. During the integration of the sinus grafts, the patient could evaluate TMJ setting, aesthetics, and function (Figure 3).
Figure 1. The patient presents in a severe Class III occlusal relationship and with a deep underbite. Maxillary right and left posterior teeth were missing, and the anterior dentition was periodontally sound.
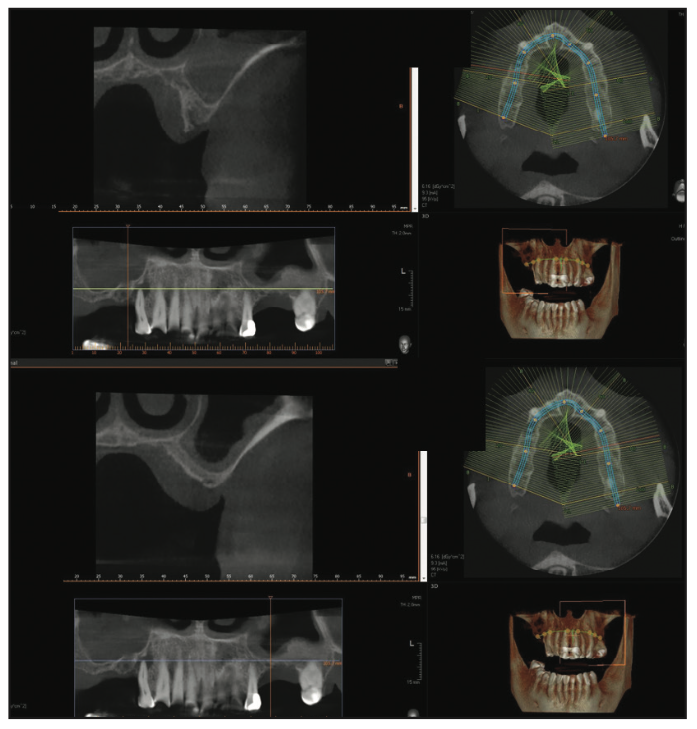
Figure 2. CBCT analysis demonstrated significant collapse of the right and left posterior sinuses.

Figure 3. Prior to any commitment to final prostheses, the maxillary right and left sinuses were augmented using the Caldwel-Luc procedure, and the remaining maxillary dentition was temporized. The severe underbite was corrected.
Proper positioning and spacing of the posterior implants were evaluated using a “tooth-first” approach. Conventional guided surgical protocols were followed, including virtual design and positioning of implants in the edentulous areas before any surgical intervention. The tooth design was determined prior to any surgical intervention, and osteotomies were performed to idealize dentition shape. For example, for a 6-mm-wide first bicuspid tooth, the pilot bur is positioned 3 mm from the adjacent tooth. The pilot osteotomy for the subsequent 7-mm second bicuspid replacement would thus be 6.5 mm from the primary pilot opening (Figure 4). The size width of the implant chosen is ideally one-half of the desired tooth width (Figure 5).6 Following 6 months of integration of the sinus grafting, a new CBCT analysis demonstrated adequate bone height and width to continue with implant placement (Figure 6).
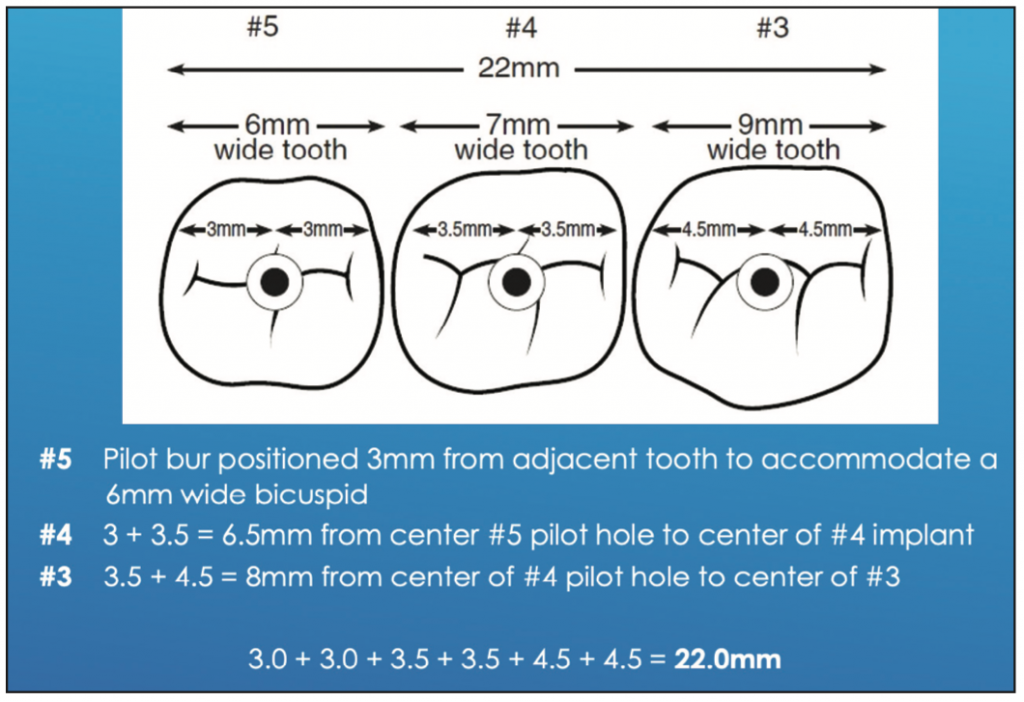
Figure 4. Proper positioning and spacing of the posterior implants was evaluated using a “tooth-first” approach. The tooth design is determined prior to any surgical intervention.
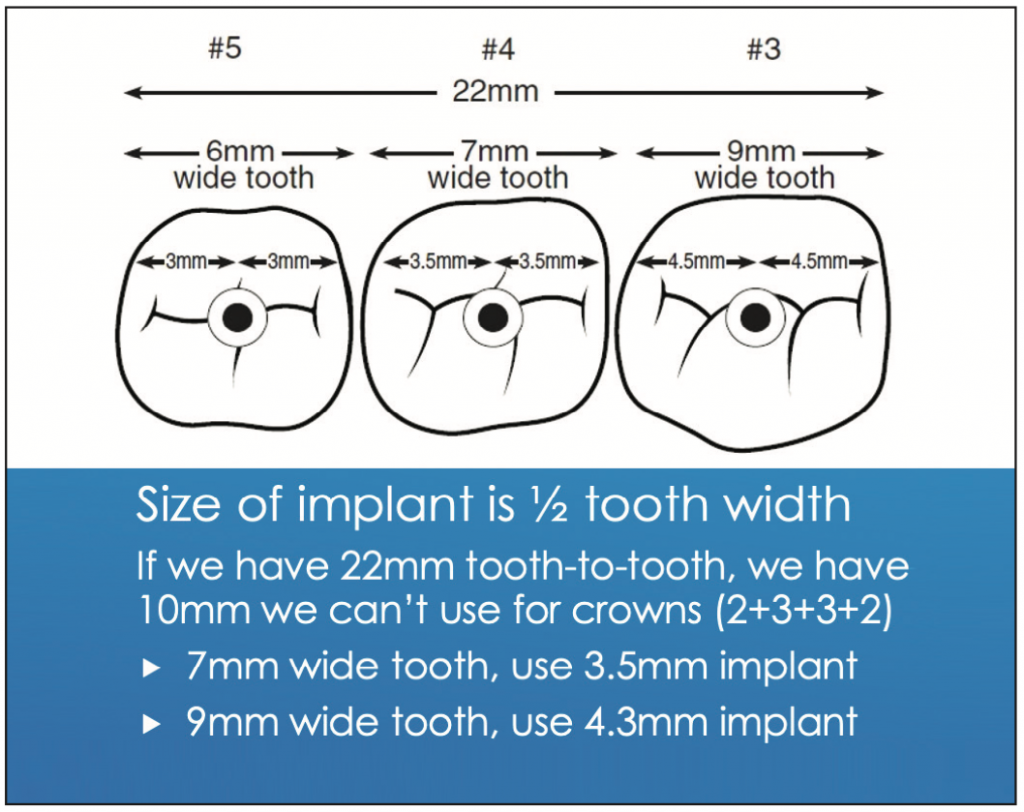
Figure 5. The size width of the implant chosen is ideally one-half of the desired tooth width.
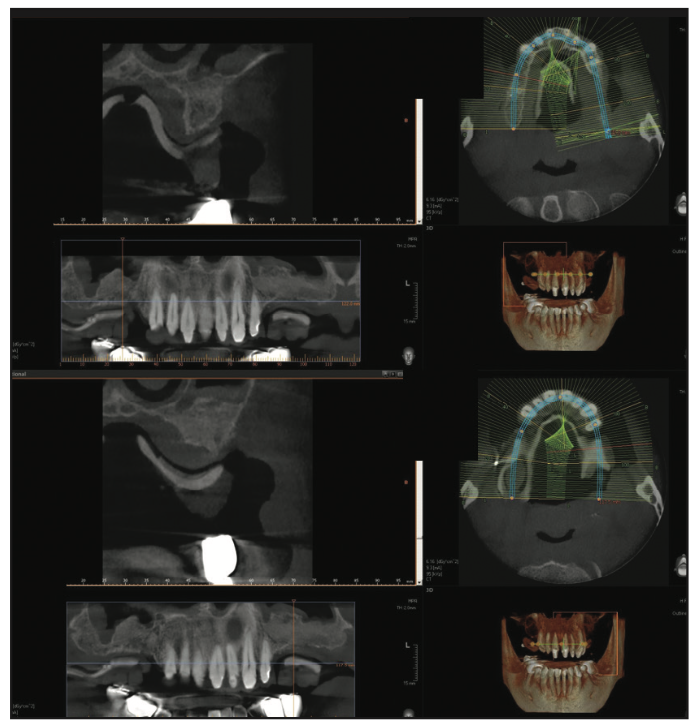
Figure 6. Following 6 months of integration of the sinus grafting, a new CBCT analysis demonstrated adequate bone height and width to continue with implant placement.
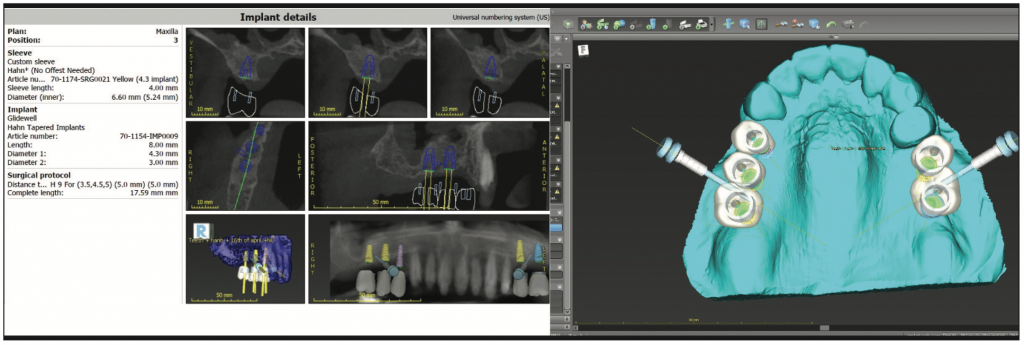
Figure 7. Guided surgical protocols were followed with an understanding of “tooth-first” restorations. Virtual design allows for fabrication of a surgical guide that aids in better positioning of the dental implants to better support the required function and predetermined aesthetics.

Figure 8. The surgical guide was both tooth- and bone-supported to maximize stability. No rocking was allowed.
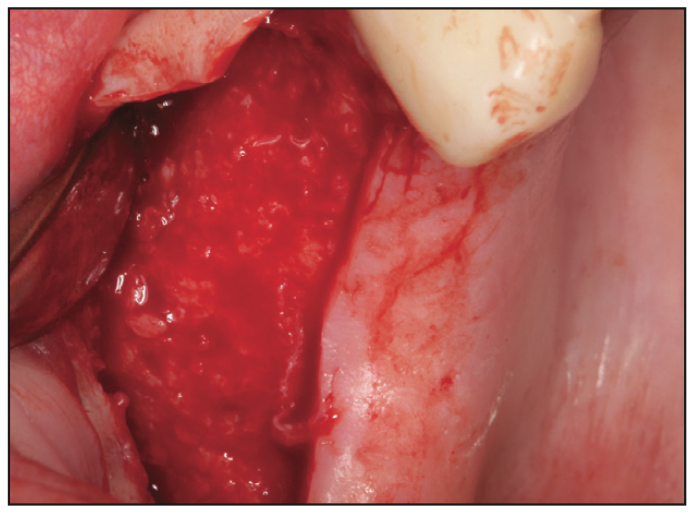
Figure 9. To ensure that the surgical guide rested on hard tissue, a complete reflection of gingiva was made, exposing the available bone.

Figure 10. Guided surgical protocol was used to make the osteotomies directly through the designed guides. This method provides for maximizing the predetermined implant position in the available bone.
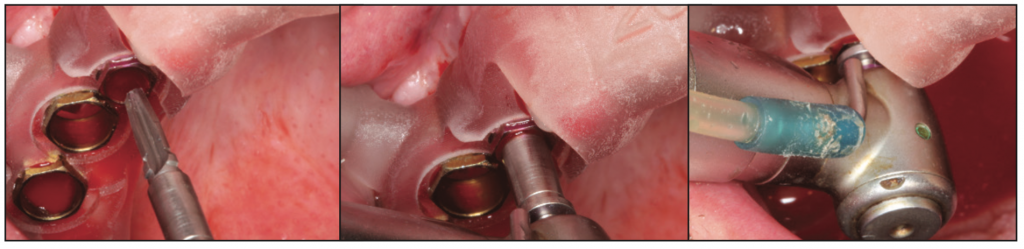
Figure 11. The osteotomies were widened using the guided burs.
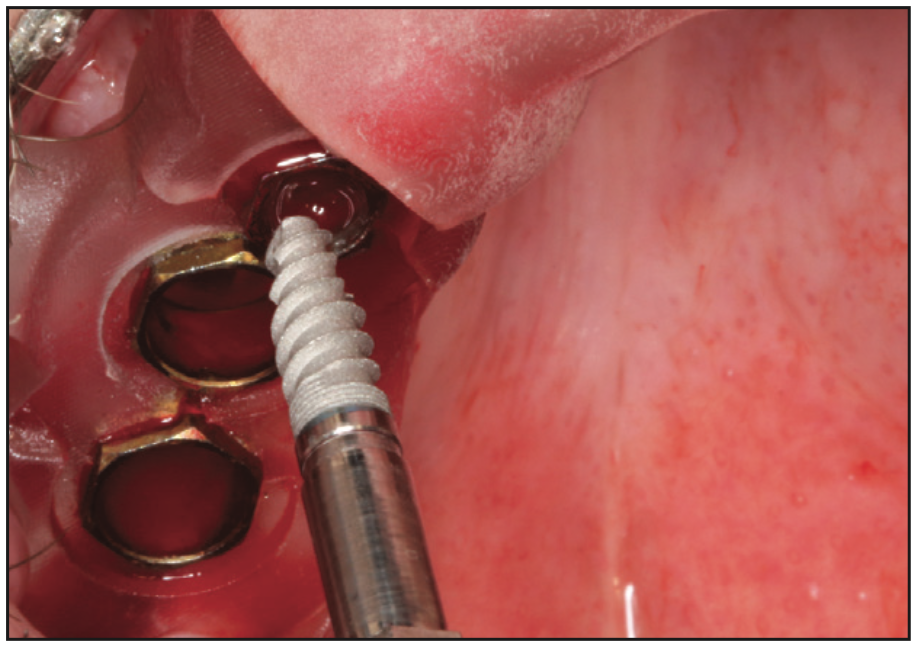
Figure 12. The Hahn Tapered Implant System (Glidewell) was torqued to position.
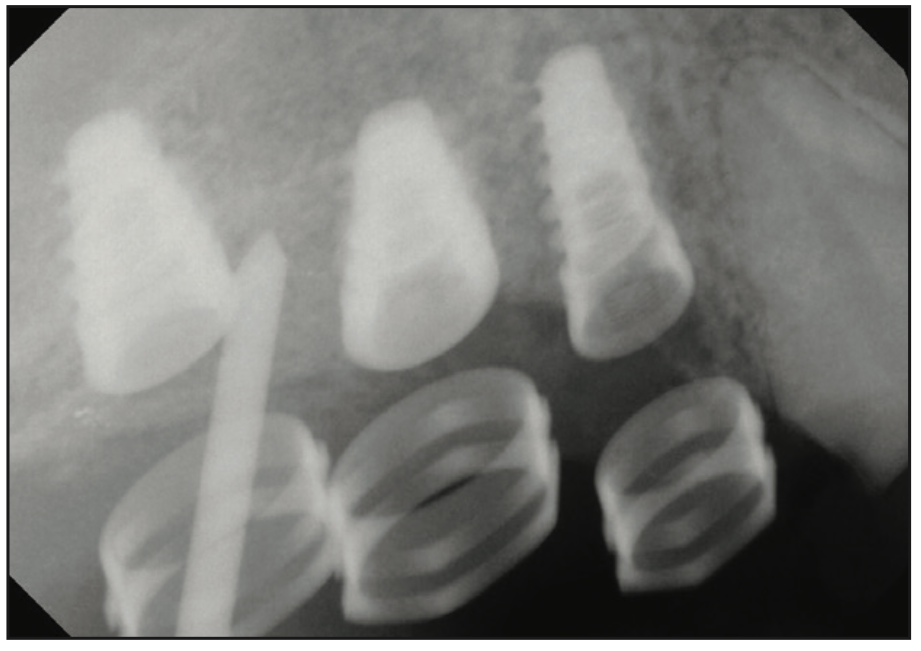
Figure 13. Digital radiographs ensured proper positioning to the crest of bone and were examined visually intraorally.
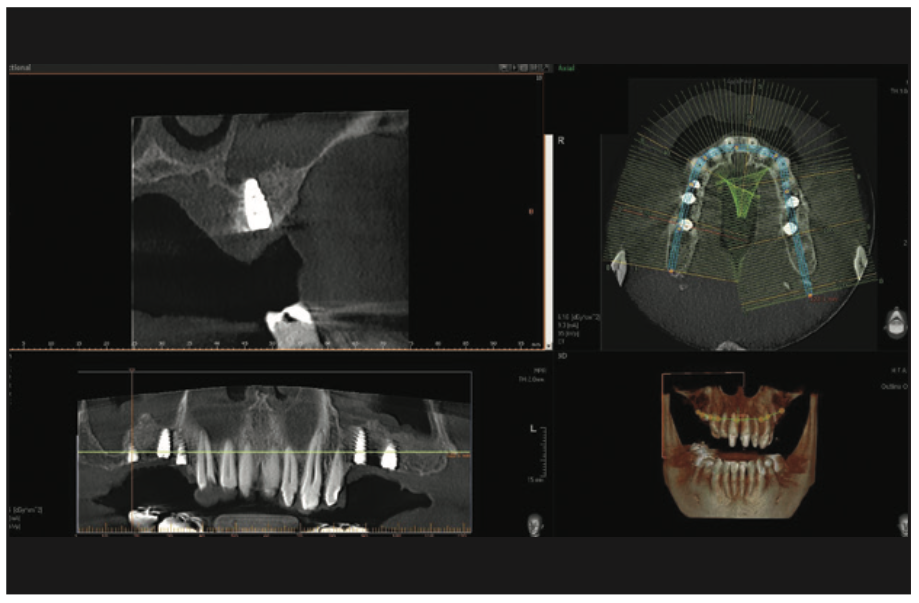
Figure 14. A final CBCT analysis was completed prior to suturing the reflections.
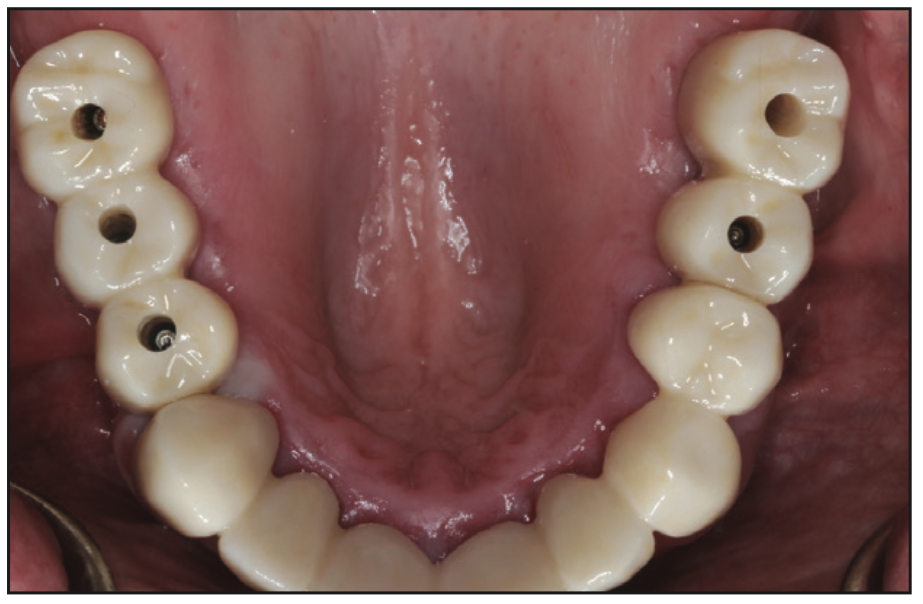
Figure 15. After integration of the implants, impression techniques were used, and the final zirconia crowns were seated to place along with the conventional splinted restorations in the anterior.
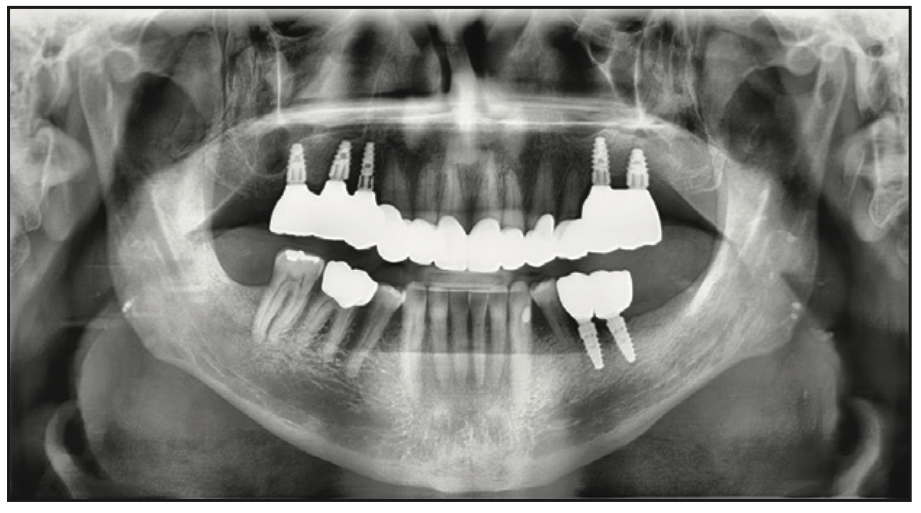
Figure 16. Full-arch restoration was completed in stages, resulting in improved aesthetics and function for the patient, meeting his expectations.

Figure 17. Images of preoperative dental relationships to transitional appliances to the final zirconia prosthetics with increased form and function.

Figure 18. Pre-op vs final smile.
Guided surgical protocols were followed with an understanding of “tooth-first” restorations. Virtual design allowed for the fabrication of a surgical guide that aided in better positioning of the dental implants to better support the required function and predetermined aesthetics (Figure 7). The surgical guide was both tooth- and bone-supported to maximize stability. No rocking was allowed. To ensure that the surgical guide rested on hard tissue, a complete reflection of the gingiva was made, exposing the available bone (Figures 8 and 9). Guided surgical protocol was used to make the osteotomies directly through the designed guides. This method provided for maximizing the predetermined implant position in the available bone. The osteotomies were widened using the guided burs (Figures 10 and 11). Figure 12 illustrates the Hahn implants torqued to position at 45 Ncm. Digital radiographs ensured proper positioning to the crest of bone and were examined visually intraorally. A final CBCT analysis was completed prior to suturing the reflections (Figures 13 and 14). After integration of the implants, impression techniques were used, and the final zirconia implant crowns were seated and placed. The splinted restorations in the anterior were also cemented (Figure 15). The full-arch restoration, screw-retained implant prostheses were completed in stages, resulting in improved aesthetics and function for the patient and meeting the patient’s expectations (Figure 16). Figures 17 and 18 illustrate the preoperative dental relationships to transitional appliances to the final zirconia prosthetics with increased form and function and the final smile design compared to the pre-op aesthetics.
CONCLUSION
Fully or partially edentulous patients are often resigned to a minimized quality of life. Function is most critical in individuals missing teeth, but creating aesthetics, emergence profile, and smile design may be equally important in their eyes. Those with natural teeth often find it challenging to imagine wearing denture teeth or losing their teeth totally, regardless of their conditions. Tooth loss results in bone loss over time, as has been discussed here. Bone loss may also occur around dental implants depending on many factors, so maintaining available hard tissue intuitively results in some semblance of insurance for any future treatment or retreatment. Implant-retained crowns and bridges allow for replacement with fixed teeth. CBCT-diagnosed and treatment planned and digitally designed restorations using custom-milled zirconia offer the most viable alternative and dramatically improve both chewing efficiency and patient quality of life. Therefore, consideration should be made to maintaining natural dentition when possible. Not every situation requires full-mouth extraction and bone contouring to achieve acceptable form and function and a long-term positive prognosis.
REFERENCES
1. Haiderali Z. The role of CBCT in implant dentistry: uses, benefits, and limitations. British Dent J. 2020;228:560–1. doi:10.1038/s41415-020-1522-x
2. Kosinski TF. Being proficient, efficient, and financially rewarded doing implant dentistry. The Profitable Dentist. 2018;4:50-67.
3. Bissasu M, Bissasu S. An intraoral method of verifying interocclusal distance for completely edentulous patients. J Prosth Dent. 2022;128(3):245–7. doi:10.1016/j.prosdent.2020.07.027
4. Kosinski TF. Dental implant hybrids for maximum esthetics: a next generation option for implant-retained prostheses. Inside Dentistry. 2015;11(5):74-80.
5. Chen P, Nikoyan L. Guided implant surgery: a technique whose time has come. Dent Clin North Am. 2021;65(1):67-80. doi:10.1016/j.cden.2020.09.005
6. Kosinski TF, Tilley S. The implant screw retained fixed detachable bridge: improving quality of life for edentulous patients. Inside Dentistry Technology. 2020;11(2):31-44.
7. Kaufman E. Maxillary sinus elevation surgery: an overview. J Esthet Restor Dent. 2003;15(5):272–82; discussion 283. doi:10.1111/j.1708-8240.2003.tb00298.x
8. Kosinski TF. Improving our patients’ quality of life: creation of the bruxzir hybrid to increase form and function. The Profitable Dentist. 2018;3:56–9.
9. Carpentieri J, Greenstein G, Cavallaro J. Hierarchy of restorative space required for different types of dental implant prostheses. J Am Dent Assoc. 2019;150(8):695-706. doi:10.1016/j.adaj.2019.04.015
10. Kosinski TF. Bone grafting: Essential indications and techniques in implant dentistry. Chairside Magazine. 2017;12(2):67-74.
11. Kosinski TF. Tooth extractions and bone grafting. Dent Today. 2018;37(9):70-75.
ABOUT THE AUTHORS
Dr. Kosinski received his DDS degree from the University of Detroit Mercy School of Dentistry (Detroit Mercy Dental) and his mastership in biochemistry from the Wayne State University School of Medicine. He is an affiliated adjunct clinical professor at Detroit Mercy Dental; serves on the editorial review board of REALITY, the information source for aesthetic dentistry; and is the past editor of the Michigan Academy of General Dentistry Update. He is currently the editor of the AGD journals General Dentistry and AGD Impact and is the editor of Implants Today for Dentistry Today. He is a past president of the Michigan AGD. He is a Diplomate of the American Board of Oral Implantology/Implant Dentistry, the International Congress of Oral Implantologists, and the American Society of Osseointegration. He is a Fellow of the American Academy of Implant Dentistry and received his Mastership in the AGD. Dr. Kosinski has published more than 220 articles on the surgical and prosthetic phases of implant dentistry and was a contributor to the textbooks Principles and Practices of Implant Dentistry and 2010’s Dental Implantation and Technology. He can be reached at drkosin@aol.com or via the website smilecreator.net.
Dr. Tilley is a graduate of the University of Alabama School of Dentistry. She is a native of Pensacola, Fla, and has been practicing dentistry in her hometown since 1998. She has done extensive training at the Las Vegas Institute for Advanced Dental Studies and the Engel Institute with Drs. Timothy Kosinski and Todd Engel. Her lectures discuss bone grafting procedures and surgical and prosthetic aspects of implant dentistry. She is a Fellow of the International College of Dentists and most recently was inducted into the American College of Dentists and the Academy of Dentistry International. She is a member of the AGD, the ADA, the Florida Dental Association, the Alabama Dental Association, the Academy of Laser Dentistry, and the Academy of American Facial Esthetics. Dr. Tilley is also a Fellow with the International Congress of Oral Implantologists. She has published extensively on implant dentistry techniques, lasers, and Botox/fillers. She can be reached via email at stephflynntilley@cox.net.
Disclosure: The authors report no disclosures.