

INTRODUCTION
Generally, an endodontic article with the above title would be one about making rotary endodontics safer, reducing the possibility of instrument separation with, perhaps, a secondary effort to discuss ways to improve the 3D cleaning and debriding of canal systems. What would not be addressed is rotary’s potential to induce microcracks in canal walls.1-4 It would be a given that the overriding advantage of rotary NiTi is the increased ability to shape curved canals with far less distortion than the use of stainless steel K-files.5,6 It would also be a given that an engine-driven system is likely to reduce the procedural time necessary to accomplish its tasks while also lowering the amount of hand fatigue the dentist will encounter. In short, the thrust of most articles of this nature is to emphasize the superiority of rotary NiTi instrumentation while ignoring negative impacts such as dentinal microcracks or declaring that they are artifacts of experimental protocols that don’t reflect clinical reality. Also, with a set of simple precautions, separation can be drastically reduced without compromising the goals of instrumentation—namely 3D cleansing and debridement and the introduction of ever newer versions of heat-treated NiTi instruments, reinforcing their already accepted use as an ongoing paradigm improvement over anything that came before it.
This article is different. It discusses the impact of the precautions necessary to maintain the integrity of rotary NiTi instruments. It then offers alternative methods of instrumentation that virtually eliminate the need for implementing those precautionary steps, giving the dentist the freedom to more thoroughly cleanse the canals three-dimensionally, rapidly, and without distortion. Let’s start with some of the more strongly suggested precautions.
STAYING CENTERED
The idea behind this precaution is to minimize the amount of flexural stress the rotary NiTi instruments are subjected to. Rotating NiTi instruments that are negotiating canals of increasing and more abrupt curvatures will unavoidably encounter flexural stresses, subjecting them to repetitive bouts of tension and compression that can lead to cyclic fatigue and instrument separation, even if they stay centered.7-9 In canals that are oval, typically having a wider dimension buccolingually than mesiodistally, one can only reach the tissue in the buccal and lingual extensions if the instruments are applied to those locations. Straight canals give the dentist some latitude in veering off center to reach these extended spaces, but an oval canal that is already curved mesiodistally subjects the rotary instruments to far greater flexural stresses if they are also applied buccolingually to remove that tissue. Experienced clinicians, as well as informed manufacturers, are aware of these stresses that have led to the implementation of the precaution to stay centered.
This precaution does not exist in a vacuum. Non-application of the instruments buccolingually leads to inadequate cleansing of oval canals and thin isthmuses, as has been demonstrated in numerous research articles over the past decades.10-12 The improvements in NiTi metallurgy have not eliminated the need to keep applying this precaution. Perhaps of greater significance is the redirection of the goals of instrumentation. It is supposed to be about 3D cleansing, but as the precaution of staying centered so clearly demonstrates, it increasingly appears that maintaining the integrity of the instruments has become more important than the cleansing of the canal. Those advocates of rotary NiTi would disagree, showing endless beautifully shaped and obturated highly curved canals mesiodistally. What is missing is any information on the quality of instrumentation and obturation in the buccolingual plane, something that we know exists because of the myriad of articles discussing this shortcoming.
From a practical point of view, despite articles saying that rotary NiTi can be used with a light brushing motion against all canal walls, anyone employing these instruments in canals significantly curved in the mesiodistal plane is unlikely to extend their use buccolingually, knowing intuitively that leaving a separated instrument glaringly visible on radiographs is simply less appealing than shaping a canal that looks great on a radiograph even though it may be inadequately prepared buccolingually (Figure 1). And we can always rationalize that the canals are probably round in cross section along their entire length. There is no evidence present to contradict this conclusion when all information is confined to the mesiodistal plane.
Figure 1. Radiograph of a separated instrument, which is rotary’s main concern.
Other precautions include routine inspection of the instruments, noting any detectable defects of unwinding or overwinding of the flutes that demand immediate discarding of the instruments. The instruments should be used with a light pecking motion to minimize torsional stresses. Single usage is highly recommended, and the motors driving the instruments should be set to a low torque setting so the engine can kick into auto-reverse, if exceeded. It goes without saying that a well-defined glide path is essential before contemplating rotary usage, particularly where canal anatomy is becoming more complex. It is important to note that the implementation of these precautions takes on greater importance as the canal anatomy becomes more challenging. The inverse of this insight is that rotary can be done relatively safely where canal anatomy is simple, namely straight canals, fairly wide in the mesiodistal plane, and again discounting the possibilities that the canal may be wider in the buccolingual plane.
The state of canal anatomy has a profound impact on the stresses that the rotary NiTi instruments are subject to, and it is imperative that dentists routinely make these distinctions. What is easily possible in a straight, fairly wide canal is likely a far greater challenge in narrow, curved, oval canals.13,14 What I have been describing up to this point are the limitations of rotary NiTi and the compromises they must make to reduce the incidence of instrument separation. This goal is so embedded in their usage that it is reasonable to say that the prevention of separation takes precedence over their cleansing action. Indeed, in recent years, we have seen the introduction of minimally prepared canals as an evolutionary step in their safe usage, defined as a lower incidence of instrument separation. More conservative instrumentation subjects the instruments to less flexural and torsional stresses because they simply encounter less resistance on the way to the apex. They reduce the number of instruments required, lowering the costs of armamentarium to the dentists. Procedural times are reduced—all pluses for the dentists. What is not considered is the exacerbation of inadequate cleaning, in general, and oval canals, in particular, in the buccolingual dimension.15 That lack of concern is consistent, however, with what is now most important to those employing rotary instrumentation, which is keeping the instruments intact.
Given this critical review of the compromises inherent in the use of rotary NiTi, what alternatives exist that do not compromise the cleansing of canals and, at the same time, don’t induce instrument separation? The answer lies in the use of stainless steel, relieved, twisted reamers employed in a 30° handpiece oscillating at 3,000 to 4,000 cycles per minute, or about 60 cycles per second (Figure 2).16 To appreciate the positive collective impact of the instruments and the handpiece, we must get into the details of their action.
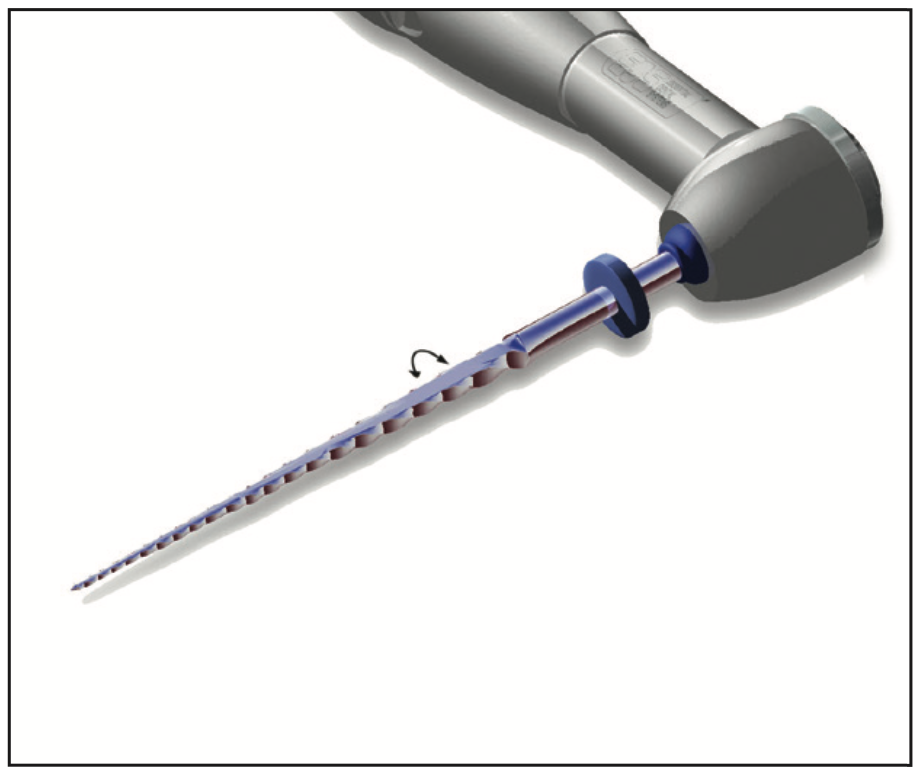
Figure 2. Illustration showing the 30° oscillating handpiece utilizing the relieved reamers.
We use reamers rather than K-files because the flutes on a reamer are twice as vertically oriented as those on a K-file. Why is that important? Dentin is only shaved away from the canal walls when the flutes of the instrument are more or less at right angles to the plane of motion. A K-file with predominantly horizontal flutes is in the same plane as the motion of an oscillating handpiece. Consequently, its function under these circumstances is to embed or screw into the dentin, penetrating the canal wall without removing any dentin up to this point, only to unscrew and repeat the process in the next cycle. Dentin is only removed when the pull motion is applied. Since the handpiece is oscillating horizontally at 3,000 to 4,000 cycles per minute, the implementation of a file design is grossly inefficient. If we substitute a reamer, its predominantly vertical flute orientation starts to shave dentin away with the first clockwise stroke. Now, admittedly, the 30° short arc of motion removes very little dentin per stroke, but at a frequency of 3,000 to 4,000 cycles per minute, or about 60 cycles per second, this automated use of a reamer is very efficient at shaping and cleansing the canals.
We further improve the mechanics by incorporating a flat along the length of the reamers, reducing their engagement with the canal walls, resulting in reduced resistance and more rapid negotiation to the apex. These instruments employed in the oscillating handpiece are used with a pecking motion—but not one concerned with exceeding the torsional limits of the metal. The 30° arc of motion is so small that it reduces the torsional stresses to which the instruments are subjected to the level of insignificance, eliminating any chances of instrument separation under these conditions. The same can be said for flexural stresses when negotiating around a curve. The repetitive, high amounts of tension and compression that a rotary instrument undergoes when negotiating significantly curved canals are reduced to insignificant amounts when the arc of motion is limited to 30°, despite the high frequency.
The most significant difference between rotary NiTi instrumentation and the 30° oscillation of relieved, stainless steel, twisted reamers is that the latter is virtually immune to separation. That fact alone stands in stark contrast to rotary instruments, where the goal of avoiding instrument separation has become the number one priority in their usage. With instrument separation a non-issue, 30° oscillating instruments are not confined to centered shaping. Limited to very rapid, short arcs of motion, the oscillating instruments can be applied aggressively buccolingually in oval canals while simultaneously negotiating highly curved canals mesiodistally (Figure 3). Their resistance to instrument separation has been verified in research studies as well as in clinical usage over many years.17
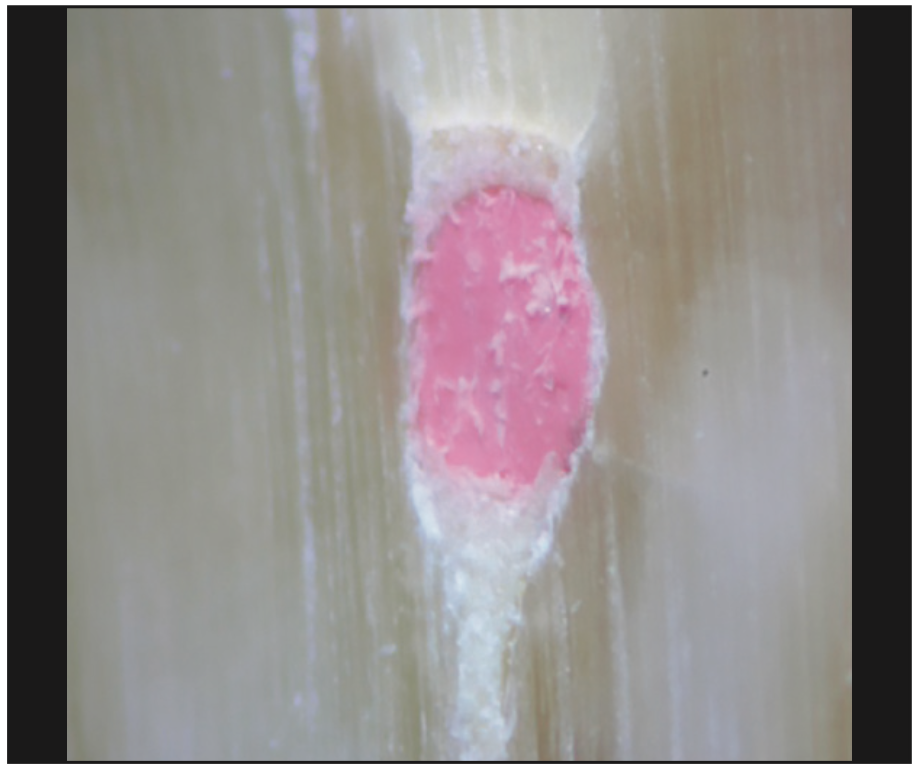
Figure 3. Photograph of the 3D cleansing that is possible with 30° oscillating reamers.
Other advantages are to be considered: Since aggressive usage does not lead to instrument separation, they may be used multiple times. It is unlikely any instrument will show signs of unwinding or overwinding when used in this manner. Confining the instruments to short arcs of motion is not only beneficial to them; it is also beneficial to maintaining the integrity of canal walls. Newton’s Third Law of Motion states that 2 interactive bodies have an equal and opposite effect on each other. We know that when confined to short arcs of motion, the impact of the canal walls on the instruments does not result in instrument separation. In like manner, the impact of the instruments on the canal walls, in accordance with Newton’s Third Law of Motion, should not result in dentinal defects. This is in stark contrast to the use of rotary NiTi instruments, which not only results in instrument separation but also in well-documented data demonstrating their production of dentinal defects at the same location where maximum stresses are produced. Ignoring these facts does not make the problem go away.
Even if a rotary NiTi enthusiast were to concede that 30° oscillating, stainless steel, relieved, twisted reamers are virtually immune to instrument separation, he or she would still argue that it is a moot point because stainless steel stiffer than NiTi is going to produce distortions to the canal walls that imperil successful endodontic instrumentation. One goal of instrumentation is to avoid the transportation of canals that can produce blunderbuss anatomy, something that is extremely difficult to obturate. The claim to superior non-distorted shaping is the final defense of rotary users, and that would be true if stainless steel were used with full rotations. However, when confined to short arcs of motion, they have been shown to remain true to canal anatomy. How can an instrument significantly stiffer than NiTi remain true no matter how short the arc of motion?
To understand this concept, we must go back in time to 1985, when Dr. James Roane published a paper describing what he called the balanced force technique using K-files.18,19 These files, however, were not used with a filing-up-and-down motion. Instead, they were employed first with a short clockwise stroke, followed by a short counterclockwise stroke, while at the same time applying an apical force to prevent the instrument from simply unscrewing. He describes employing the K-files with a reamer (horizontal) action. The counterclockwise motion cleaves off the dentin that was engaged in the initial clockwise motion. The secret to non-distortion lies in the fact that, confined to short arcs of motion, the resistance of the canal walls to deformation is greater than the tip of the stainless steel instruments. When the tip of the instrument contacts the canal walls in a curved canal, it is the instrument that is being deflected into the pathway of least resistance, which is the patent canal pathway. The same instrument used in full rotation would likely cause a ledge and lead to the distortions that are to be avoided. The reamers being relieved with the flat side along their entire working lengths are more flexible, further improving their adaptability to any canal curvatures they encounter.
So, what do we have up until this point as an alternative to rotary NiTi? We have a method of instrumentation that virtually avoids separation, and because we no longer have separation as a cause of concern, we have a method that can be vigorously applied to all the canal walls, including oval canals and thin isthmuses. We have a system that is fully automated from the first instrument that enters the canal to the last, essentially eliminating all hand fatigue, including the creation of the glide path. It is a system that is far less likely to produce dentinal defects. The instruments can be used multiple times with significant cost savings. From my perspective, the elimination of instrument separation takes away the greatest source of anxiety and lets us address what should truly be our main goal: the improved ability to thoroughly cleanse the canals in 3 dimensions without distortion.
Practical Application
This alternative method of instrumenting canals sounds good, but how does it work in practice? Let’s take a typical mandibular molar to see how we apply the mechanics from start to finish. After giving the appropriate anesthesia—in my case, 2 mandibular blocks, the first with carbocaine, followed by xylocaine 1/100m, and then augmented with intraligamentary injections using articaine—I apply the rubber dam over a #4 clamp. I then gain access under the microscope to the pulp chamber, generally using a long-shank, high-speed #4 round bur. If I am lucky, a non-calcified pulp chamber is present, and I quickly debride it of pulp tissue using slow-speed #3 and #2 Munce Discovery Burs (CJM Engineering). Once I detect the canal orifices, I generally apply 6% NaOCl if the case is non-vital or 17% EDTA if it is vital or at least partially vital. At this point, I generally take a 25-mm 06/02 stainless steel reamer into the MB canal and negotiate it manually to the length of the canal using the apex locator as my measuring device. This reamer is so thin and flexible that it generally negotiates to the apex with minimal resistance. If the canals are somewhat calcified and I meet significant resistance to deeper penetration, I will always then apply 17% EDTA and place the 06/02 reamer in the oscillating handpiece. This greatly facilitates negotiating the instrument to the apex. I then confirm the correct length via the apex locator. In this manner, I gain the lengths of the canals that are present—typically 3, sometimes 4—and generally use the MB cusp as my reference point for length.
Once I have negotiated to length via the 30° oscillating handpiece, I work the instrument vigorously against the buccal and lingual walls of all the canals. If any of the canals are oval in nature or an isthmus is present, the shaving of dentin in these wider dimensions will be visually apparent after about 5 seconds of application. Interestingly, a canal that is tight and offers resistance to a 06/02 stainless steel twisted reamer always encounters less resistance when I skip to the 10/02 to further widen the canals, clearly demonstrating the effectiveness of the initial instrument having the ability to effectively shave dentin away from the canal walls. Its thin dimensions give it the freedom of greater penetration, and the 30° oscillations, combined with its high frequency of use, make it a perfect instrument for what I call “internal routing,” the enlargement of the canal space beyond the dimensions of the instrument being used to shape the canals. In this manner, I tend to enlarge the canal spaces typically to a 35/02, always flooding the canals with irrigant, be it NaOCl, EDTA, or Irritrol, a combination of EDTA and CHX that efficiently kills any bacteria that may be remaining in the canals. The combination of irrigant and physical contact of the canal walls tends to remove adherent biofilms that would be resistant to irrigants alone.
Not all canals are opened to 35/02. In particularly long, tortuous canals that are extremely narrow to start with, I may elect to limit enlargement to a 30/02. If that is the case, it still does not prevent me from working the instruments aggressively buccolingually for improved debridement. In either case, I am not quite done with the instrumentation. As much as I am wary of rotary NiTi, it has 2 advantages of which I take advantage: (1) It smoothes the canal walls in the mesio-distal plane, and (2) it sizes the canal at least mesiodistally for the appropriate gutta-percha point. If opened to a 35/02, I follow up with a 30/04 rotary, and if limited to a 30/02 preparation, I will then take a 30/02 rotary and negotiate to the apex.
However, it should be clearly understood that when I apply rotary NiTi, I have already cleansed the canals, possibly oval with thin isthmuses, with the oscillating, stainless steel, relieved reamers. If I encounter anything that I interpret as excessive resistance when using the rotary system, I will further enlarge the canals with the stainless steel, oscillating reamers to the point where the resistance is minimal. In that way, I have not separated a rotary instrument in years. I should add that we developed helically relieved rotary NiTi instruments that, because of the relief, encounter less resistance when negotiating to the apex. These particular relieved NiTi reamers minimize the possibility that the canals will require further enlargement before they can safely reach the apex.
That pretty much takes care of the mechanics prior to obturation. Figures 4 to 9 illustrate a number of cases that I have treated, showing the adaptability that this approach offers the dentist in achieving results that would entail more risk if they were done predominantly with rotary NiTi.
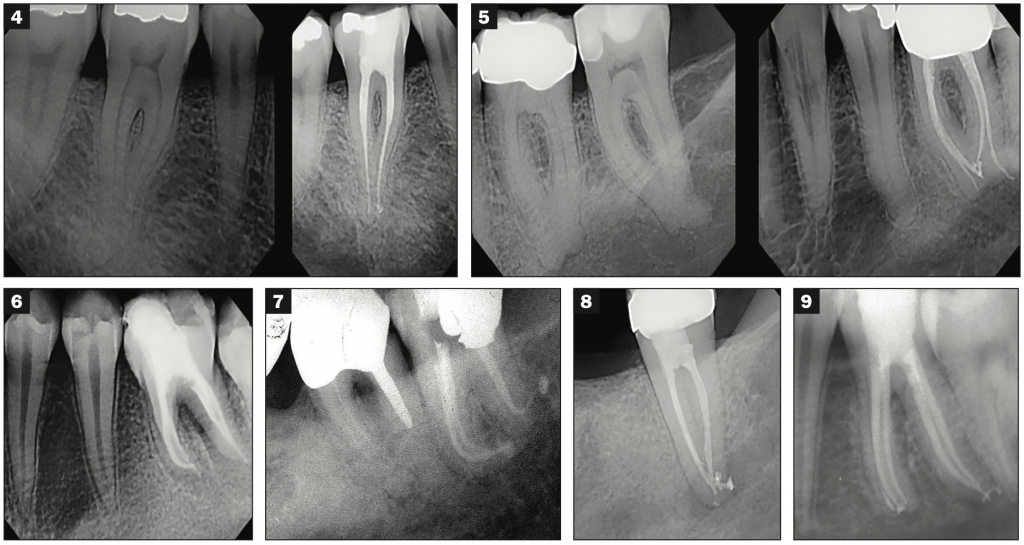
Figures 4 to 9. Examples of canal instrumentation and obturation following 30° oscillation with no more than one final rotary instrument smoothing the walls and preparing the canal, at least mesiodistally, for the appropriate gutta-percha point.
CONCLUSION
The marketing of rotary NiTi instrumentation has been so ubiquitous that it has been accepted as the norm, with any deviation from that approach ridiculed as retrogressive. Yet, devotion to this approach is intimately tied to compromises that have been thoroughly diagnosed and documented in the endodontic literature and, in my opinion, needlessly inhibit the implementation of techniques readily available to the dentist and specialist alike. Alternate engine-driven non-rotary systems will tend to eliminate the stresses and uncertainty that are ever present with the extensive reliance on rotary instrumentation.
REFERENCES
1. Adorno CG, Yoshioka T, Suda H. The effect of root preparation technique and instrumentation length on the development of apical root cracks. J Endod. 2009;35(3):389–92. doi:10.1016/j.joen.2008.12.008
2. Adorno CG, Yoshioka T, Suda H. Crack initiation on the apical root surface caused by three different nickel-titanium rotary files at different working lengths. J Endod. 2011;37(4):522–5. doi:10.1016/j.joen.2010.12.002
3. Bier CA, Shemesh H, Tanomaru-Filho M, et al. The ability of different nickel-titanium rotary instruments to induce dentinal damage during canal preparation. J Endod. 2009;35(2):236–8. doi:10.1016/j.joen.2008.10.021
4. Bürklein S, Tsotsis P, Schäfer E. Incidence of dentinal defects after root canal preparation: reciprocating versus rotary instrumentation. J Endod. 2013;39(4):501–4. doi:10.1016/j.joen.2012.11.045
5. Cheung GS, Liu CS. A retrospective study of endodontic treatment outcome between nickel-titanium rotary and stainless steel hand filing techniques. J Endod. 2009;35(7):938–43. doi:10.1016/j.joen.2009.04.016
6. Pettiette MT, Delano EO, Trope M. Evaluation of success rate of endodontic treatment performed by students with stainless-steel K-files and nickel-titanium hand files. J Endod. 2001;27(2):124–7. doi:10.1097/00004770-200102000-00017
7. Bahcall JK, Carp S, Miner M, et al. The causes, prevention, and clinical management of broken endodontic rotary files. Dent Today. 2005;24(11):74, 76, 78-80; quiz 80.
8. Bahcall JK. Remedying and preventing endodontic rotary nickel-titanium (NiTi) file breakage. Compend Contin Educ Dent. 2013;34(5):324–7; quiz 328.
9. Madarati AA, Watts DC, Qualtrough AJ. Factors contributing to the separation of endodontic files. Br Dent J. 2008;204(5):241–5. doi:10.1038/bdj.2008.152
10. Peters OA, Schönenberger K, Laib A. Effects of four Ni-Ti preparation techniques on root canal geometry assessed by micro computed tomography. Int Endod J. 2001;34(3):221–30. doi:10.1046/j.1365-2591.2001.00373.x
11. Versiani MA, Leoni GB, Steier L, et al. Micro-computed tomography study of oval-shaped canals prepared with the self-adjusting file, Reciproc, WaveOne, and ProTaper universal systems. J Endod. 2013;39(8):1060–6. doi:10.1016/j.joen.2013.04.009
12. Cheung LH, Cheung GS. Evaluation of a rotary instrumentation method for C-shaped canals with micro-computed tomography. J Endod. 2008;34(10):1233–8. doi:10.1016/j.joen.2008.07.015
13. Iqbal MK, Kohli MR, Kim JS. A retrospective clinical study of incidence of root canal instrument separation in an endodontics graduate program: a PennEndo database study. J Endod. 2006;32(11):1048–52. doi:10.1016/j.joen.2006.03.001
14. Martín B, Zelada G, Varela P, et al. Factors influencing the fracture of nickel-titanium rotary instruments. Int Endod J. 2003;36(4):262–6. doi:10.1046/j.1365-2591.2003.00630.x
15. Shabbir J, Zehra T, Najmi N, et al. Access cavity preparations: classification and literature review of traditional and minimally invasive endodontic access cavity designs. J Endod. 2021;47(8):1229–44. doi:10.1016/j.joen.2021.05.007
16. Wan J, Rasimick BJ, Musikant BL, et al. Cutting efficiency of 3 different instrument designs used in reciprocation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109(5):e82-5. doi:10.1016/j.tripleo.2009.12.037
17. Wan J, Rasimick BJ, Musikant BL, et al. A comparison of cyclic fatigue resistance in reciprocating and rotary nickel-titanium instruments. Aust Endod J. 2011;37(3):122–7. doi:10.1111/j.1747-4477.2010.00222.x
18. Kyomen SM, Caputo AA, White SN. Critical analysis of the balanced force technique in endodontics. J Endod. 1994l;20(7):332–7. doi:10.1016/S0099-2399(06)80095-6
19. Charles TJ, Charles JE. The ‘balanced force’ concept for instrumentation of curved canals revisited. Int Endod J. 1998;31(3):166–72. doi: 10.1046/j.1365-2591.1998.00137.x
ABOUT THE AUTHOR
Dr. Musikant has lectured worldwide in more than 150 locations and has coauthored more than 300 dental articles published in major dental journals. As a partner in a New York City endodontic practice, his 40-plus years of clinical experience have crafted him into one of the top authorities in endodontics. He can be reached at (888) 542-6376, via email at info@essentialseminars.org, or via the website essentialseminars.org.
Disclosure: Dr. Musikant is director and co-founder of Essential Dental Systems.