
Search results
The search revealed a total of 2328 records from databases and 19 through other sources. After the removal of duplicates, titles abstracts of 1301 of them were screened, which resulted in 32 articles for full text assessment. Final scrutiny resulted in the inclusion of eight articles in the SR13,14,15,16,17,18,19,20. The details of search results, excluded studies and the reasons for exclusion are given in Fig. 1 and the online Supplementary Information.

The details of the searches, scrutiny and selection, along with the reasons for the exclusion.
Quality assessment
Risk of bias was found to be low in all the studies except Ahmed et al. which had moderate risk20. The paucities regarding the strategies to deal with confounding factors were identified in four studies13,15,17,20 and a lack of clarity regarding inclusion criteria was seen in one study (Table 2)20.
Study characteristics
The studies had been published between 2014 to 2020 with three from 202018,19,20. Among them, three had been performed in Saudi Arabia17,18,20, two in India13,15, and one each in Kuwait16, United Arab Emirates19 and Brazil14. All the studies except Murali et al.13 and Costa et al.14 were cross-sectional in design15,16,17,18,19,20. All the studies reported a lack of awareness and inadequate knowledge among parents regarding the management of dental trauma and/or dental avulsion (Table 3)13,14,15,16,17,18,19,20.
Questionnaire characteristics
The mode of distribution of the questionnaire in the majority of studies was self-administration16,17,18,20, followed by personal interviews in two studies13,14. The mode of distribution was not mentioned in the two studies15,19. The questionnaire was available in two or more languages in three studies13,15,19, one language in two studies16,18. English language was the main language in three studies and used in combination with Tamil13, Hindi, and Bengali15 and Arabic19, Arabic had also been used in two other studies16,18. The sources of Questionnaires had been mentioned in only three studies15,16,18. The questionnaires had used objective questions13,14,15,16,17,18,20 while this detail was not available in one study (online Supplementary Information)19. The knowledge of parents was assessed by all the studies except one which evaluated the perception of parents14. Along with this, the attitude was evaluated in three studies13,15,18 and practice in one study13. The number of questions varied from 5 to 3313,14,15,16,17,18,19,20, the validity was not reported in three studies15,17,19 and reliability was not reported in one study (online Supplementary Information)13.
Sampling characteristics
The sampling strategy had not been mentioned in four studies13,14,15,20 while others had simple random (n = 2)16,19, stratified cluster random (n = 1)17, and convenience sampling (n = 1)18. The sample size had been statistically justified in four studies16,18,19,20 and it ranged from 15013 to 336717 parents. The parents had been recruited from the out-patient departments (OPD) (n = 2)13,15, health care centers (PHC) (n = 2)14,17, dental specialty centers (n = 3)17,18,19 and directly from the community in one study20. Five studies had included both the parents15,16,18,19,20 whereas the other three had been done in mothers13,14,17. There was variability in the age groups of parents, however, the majority of them ranged between 20–40 years. Costa et al14 included 15–18 years old pregnant women as one of the groups while three of them had an age category of 51–60 years too13,19,20. The marital status, details of off-springs and employment status had been mentioned in the study done by Al-Sehaibany et al.17 and Alharbi et al.18. Most of the parents were married with two children in both the studies17,18. Large number of parents were working (n = 244) in the study done by Al-Sehaibany et al.17 while Alharbi et al.18 had reported that most of the parents were unemployed (n = 2503). The majority of the parents were graduates or had a professional degree in four of the included studies16,17,18,19 while the education level was less than graduation in the other four studies13,14,15,16. The details of socio-economic status were given in two studies and it was reported as middle income status (online Supplementary Information)17,18.
Details of the questions
The questions included in three or more studies were used for making the “KAP-Heat Map” (Fig. 2). It was observed that 25–50% of the parents had witnessed any form of TDI in three15,18,20 and 50–75% in two of the six studies which included this question14,17. While only 4.7% of parents had witnessed it in one study13. When the parents had been enquired whether they had obtained any information about TDI in past, three of the four studies which included this question reported that 25–50% of the parents had responded in affirmation15,17,19 while it was <25% in the study done by Alyahya et al.16. The source was reported as a dentist in Alyahya et al.16 and Al-Sehaibany et al.17, while the information was obtained by “friends” in Alharbi et al. (online Supplementary Information)18. The appropriateness of immediate action after avulsion of tooth was correctly responded by 50–75% of the parents in four of the five studies15,17,18,19 and 25–50% in Murali et al.13. Three of the included studies had enquired about parent’s ability to identify the injured tooth with two studies reporting the correct response rates as 25–50%15,17 and 50–75 % in one study each20. Correct method of cleaning the soiled avulsed tooth was enquired in four studies and was known to 25–50% of the parents in three15,16,18 and 50–75% in one study13. When the parents were asked if they can perform the replantation of the avulsed tooth in their child, <25% of them responded in affirmation in two15,19 and 25–50% in the other two studies which included this question16,20. Awareness regarding the immediate or early replantation of avulsed tooth was known to 25–50% of the parents in all the three studies which had enquired about it16,17,18. Similarly, <25% of them were aware of the appropriate storage medium for the avulsed tooth in five15,16,17,19,20 and 25–50% in two of the seven studies which had enquired about it18,20. The question about the urgency to seek professional advice after TDI was included in five studies with 50–75% of the parents replying correctly in three studies13,16,18 more than 75% in one study15 and 25–50% in one study20. Dentists were reported as the first choice of the professionals to be contacted after TDI by >75% of the parents in three of the four studies which enquired about it15,16,18. It was 25–50% in the study done by Ahmed et al.20. More than 75% of the parents in all three studies which enquired about it, reported that they wanted to obtain more information about the management of TDI (Fig. 2)15,17,20. The questions included only in one or two studies have been detailed separately in the online Supplementary Information. The majority of parents responded negatively when asked “What did you do for the trauma?”20, “Can you identify the type of tooth injury?”14, “Have you (mother) ever had any dental trauma?”13 in one study each.

The question stems included in 3 or more studies (Blue: question not included, red: > 75%, dark yellow: 50–75%, lemon yellow: 25–50%, light yellow: < 25% sports persons and coaches giving correct responses. Width of columns was proportional to the number of studies which included the question stems.
Meta-analysis
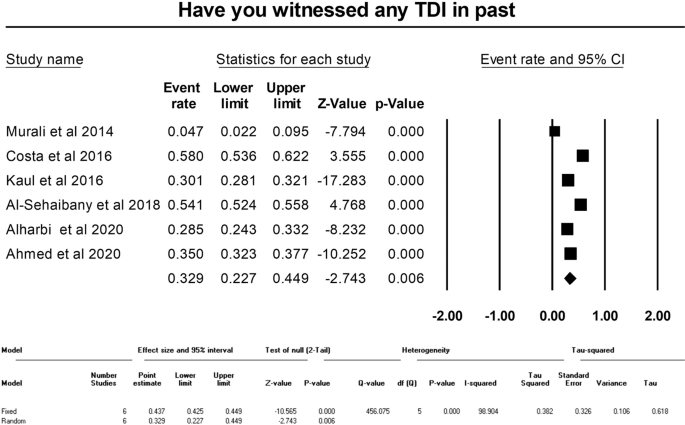
Meta-analysis could be performed for three of the questions regarding witnessing of TDI in past, immediate action after tooth avulsion, and best storage media for storage of avulsed tooth. The pooled percentage of affirmative responses of the parents regarding witnessing TDI was 32.9% (95% CI: 22.7–44.9, random effects model, p = 0.006) (Fig. 3). The immediate action after tooth avulsion was known to 54.5% (95% CI: 50.2–58.8, random effects model, p = 0.042) of the parents (Fig. 4). The appropriate response rate regarding the storage medium for the avulsed permanent tooth was 21.3% (95% CI: 16.8–26.5, Random effects model, p < 0.001) (Fig. 5). All the meta-analyses displayed significant heterogeneity (I2 values ranging from 90.33 to 98.90) and publication bias (depicted in the Funnel plots and Egger’s test) (Figs. 3–5, online Supplementary Information).
The pooled correct response percentage for question regarding best storage media for storage of avulsed tooth.
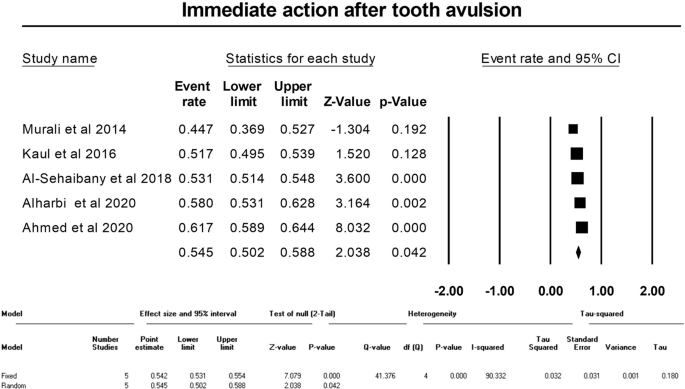
The pooled correct response percentage for question regarding immediate action after tooth avulsion.
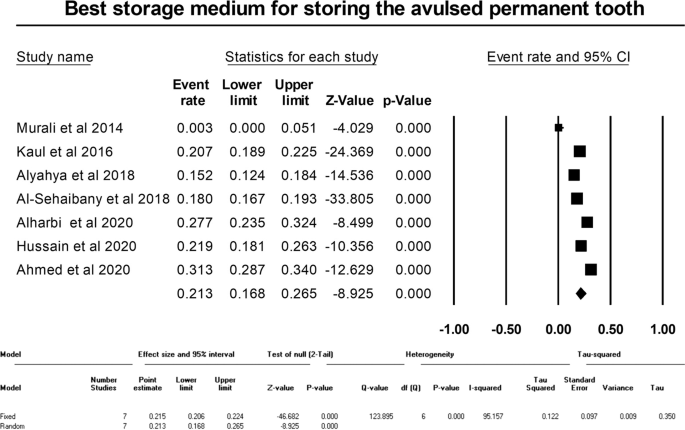
showing the pooled correct response percentage for question regarding best storage media for storage of avulsed tooth.
Grading of evidence
The strength of evidence regarding the outcomes of all the meta-analyses was graded to be very low (Table 4). This was done on the basis of the non-randomized nature of the included studies, the presence of heterogeneity, the presence of imprecision, the presence of publication bias and the presence of plausible confounding factors.