

INTRODUCTION
Crowded dentition, the result of underdeveloped jaws, can create instability in the occlusion, and this can lead to symptomatic TMJ and/or facial muscle tension. This restrictive dentition arrangement can also have a deleterious effect on the airway,1 sleep, and breathing.
In this article, a case will be presented of crowded dental arches resulting in facial muscle symptoms as well as less-than-ideal airway dimensions. The case was treated with expansive clear aligner therapy followed by minimally invasive additive composite occlusal rehabilitation.
While expansive orthodontics and occlusal rehabilitation are not, per se, a treatment for sleep-disordered breathing, this case illustrates that airway-centered orthodontic and restorative techniques enhance and stabilize the occlusion. Still, they can have a positive effect on the functional airway space.
Factors that should be considered when treatment planning a full-mouth rejuvenation are functional airway space, the stability of the TMJ, the interarch relationship (including VDO), the condition of the teeth, and the patient’s aesthetic desires.2
Airway
When treatment planning the full-mouth rehabilitation case, the airway must be given attention. Research by Simmons and Prehn3 has shown a strong correlation between nocturnal bruxism and obstructive sleep apnea. If obstructive sleep apnea is suspected, then a proper referral is first in order, and the OSA should be treated prior to starting full-mouth rehabilitation. In this manner, the patient is healthier, much less likely to brux during sleep, and will respond better to treatment. In this case study, the patient did not have OSA.
TMJ
A stable, non-symptomatic TMJ should be achieved before full-mouth restoration. If the TMJ is symptomatic, there are a variety of treatments available to stabilize it. These are not covered in the scope of this article; however, the importance of a stable, non-symptomatic TMJ should not be overlooked.
Interarch Relationship
For ideal restorative results, the teeth should be in an Angle Class I relationship. A knowledge of VDO and how it might affect the airway is important. Sagittal development of the mandible influences the pharyngeal airway passage.4,5 The author believes that the more obtuse the mandibular angle, the more likely an increase in the VDO might negatively affect functional airway space (Figure 1). So the mandibular angle should be considered when changing the VDO. It is also necessary in some cases, such as this one, to increase the VDO to allow room for proper tooth anatomy.
Figure 1. Increasing the VDO in patients with a narrow mandibular angle is likely to negatively affect the airway space than in those with a wide mandibular angle.
Condition of Teeth
Our goal for a final restorative outcome is a biologically sound chewing system with neuromuscular harmony; a healthy, stable TMJ; and natural biological tooth form.6
CASE REPORT
A healthy 60-year-old male (Figure 2a) presented with the chief complaint that his teeth were crowded and worn. He was unhappy with the appearance of his teeth and smile (Figure 2b). He also complained of facial muscle fatigue and tension. The patient denied nocturnal bruxism, but he did find himself clenching during the day. He was not taking any medications other than a daily multivitamin. No systemic medical issues or conditions were present. The patient did admit that he snores.
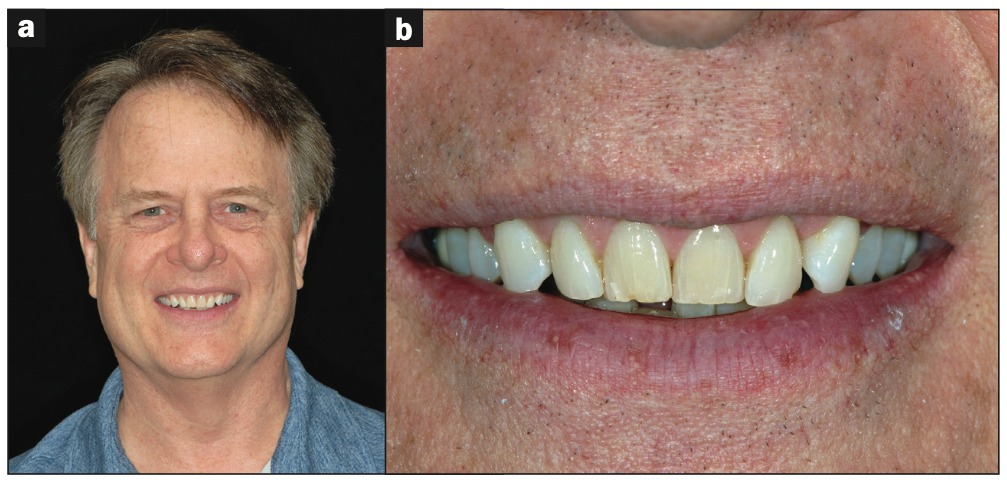
Figure 2. (a) A 60-year-old male patient. (b) He was unhappy with the appearance of his smile.
Upon completion of a thorough clinical examination and complete records, including FMX, full-field-of-view CBCT, diagnostic models, and photos, a comprehensive review of the case was done.
Findings
The patient’s tongue was not scalloped; he had a Mallampatti score of 2 and an Epworth score of 1. The CBCT showed a minimally restricted area of 206 mm2 and a total airway volume of 13.2 cm3 (Figure 3). He did not have any TMJ pain, noises, or crepitus. His maximum opening was within normal limits with no mandibular deviation. The patient’s condyles were asymptomatic but distally positioned, as seen in the CBCT (Figure 4). The masseter muscles were hypertrophic and sore to palpation. Moderate to severe enamel attrition (Figure 5) resulted in a decreased vertical dimension of 10 mm (Figure 6).
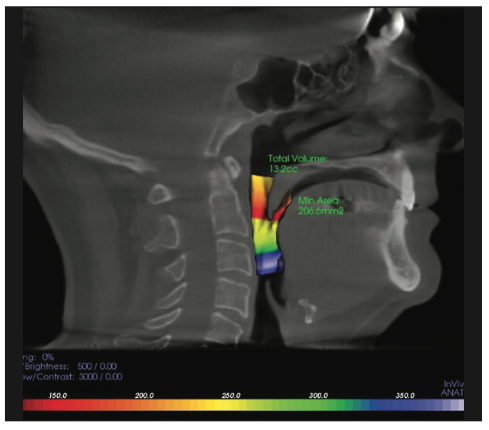
Figure 3. The preoperative CBCT shows a minimally restricted area of the functional airway of 206 mm2 with a total volume of 313.1cm3.
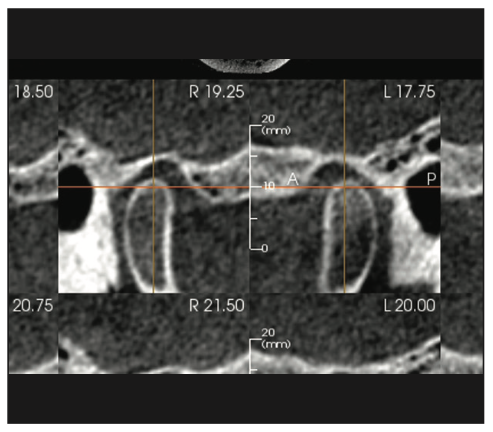
Figure 4. The CBCT sagittal view shows both condyles were distally positioned.

Figure 5. The anterior teeth exhibited moderate to severe attrition.
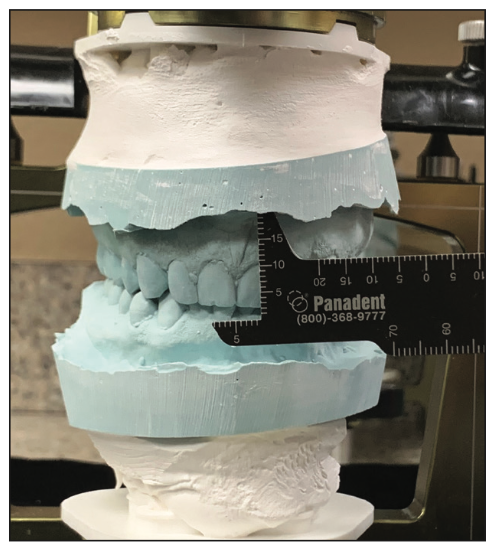
Figure 6. The pre-op VDO measured from CEJ No. 9 to CEJ No. 24. Note the passive eruption of lower incisors.
Passive eruption of the mandibular incisors was taken into consideration. Periodontal health was excellent, and no dental caries were found. Teeth Nos. 4 and 5 had old composites in need of replacement. All other existing restorations were in decent shape. Teeth Nos. 3, 14, and 19 had zirconia crowns that had poor marginal integrity. Teeth Nos. 3 and 14 had been treated endodontically. Tooth No. 15 was an implant with a PFMC. Tooth No. 31 was an implant with a zirconia crown. Teeth Nos. 1, 17, and 32 were missing. The lower anterior teeth were crowded and worn. The overjet was 0.5 mm, and the overbite was 4.0 mm. Lingual mandibular tori were present.
Clear Aligner Therapy

Figure 7. (a) Above pre-ortho maxillary teeth. (b) Below post-ortho maxillary teeth. (c) Pre-ortho maxillary occlusal view. (d) Post-ortho maxillary occlusal view.
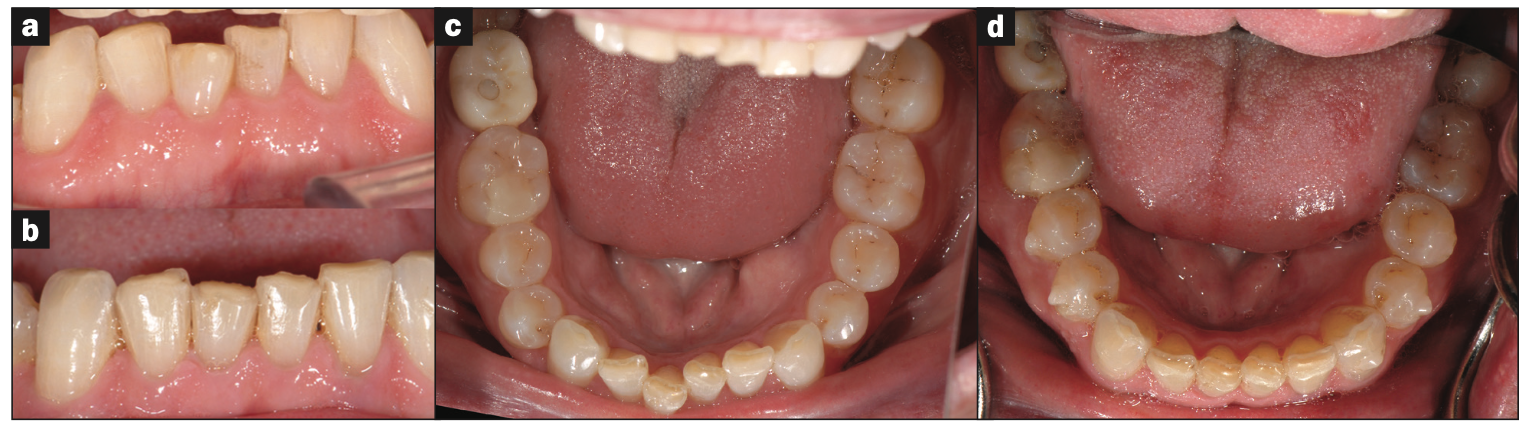
Figure 8. (a) Above pre-ortho mandibular teeth. (b) Below post-ortho mandibular teeth. (c) Pre-ortho mandibular occlusal view. (d) Post-ortho mandibular occlusal view.

Figure 9. Post-ortho improved interarch relationship.
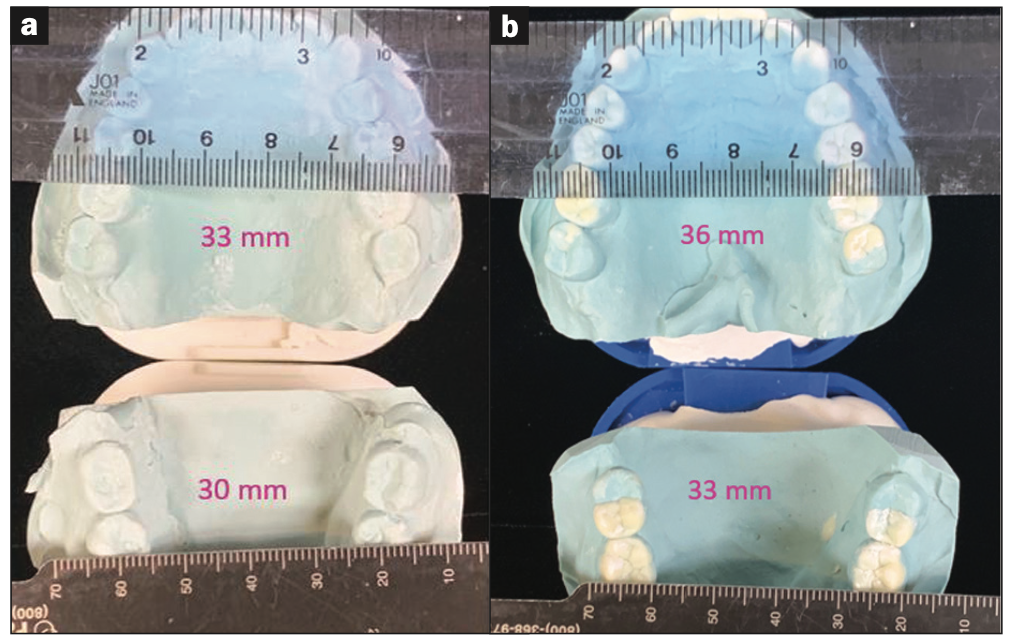
Figure 10. (a) Pre-ortho model measurements: maxillary intermolar width was 33 mm. Mandibular intermolar width was 30 mm. (b) Post-ortho model measurements: maxillary intermolar width was 36 mm. Mandibular intermolar width was 33 mm. There were net width increases of 3 mm in both arches.
Expansive clear aligner therapy was implemented to relieve the crowding in the lower anterior teeth (Figures 7 and 8) and to provide for a more ideal interarch relationship (Figure 9). Upon completion of aligner therapy, there was a transverse width increase of 3.0 mm in both the upper and lower arches (Figure 10). This created more space for the tongue. The patient was now ready for phase 2 full-mouth restorations.
Composite Bio-Rejuvenation
An open bite record was taken with an AD2 (Advanced Dental Design) bite tray at a vertical dimension that would allow the dentition to be restored with proper tooth form, overjet, overbite, and ideal centric contacts. This VDO was evaluated with a 0.75 clear retainer with an anterior acrylic stop. The patient’s comfort and facial aesthetics were analyzed with this jig in place (Figure 11).

Figure 11. With the VDO jig in, note the relaxed facial muscles, improved lip pos- ture, and that the masseters are no longer hypertrophied.
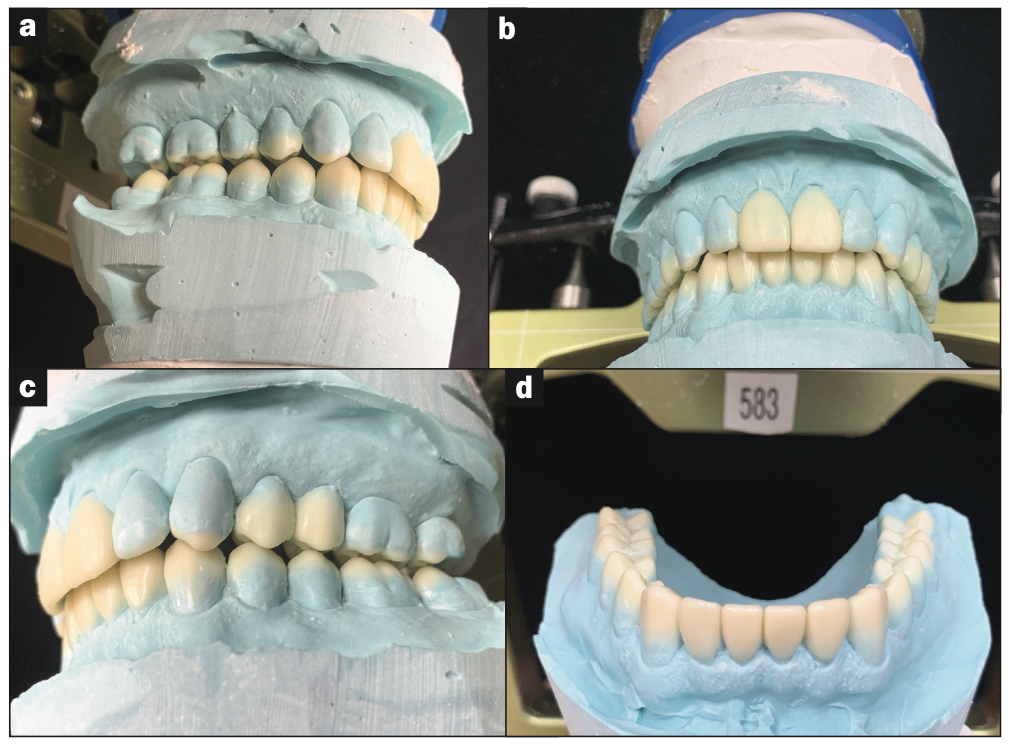
Figure 12. Final biologic wax-up.
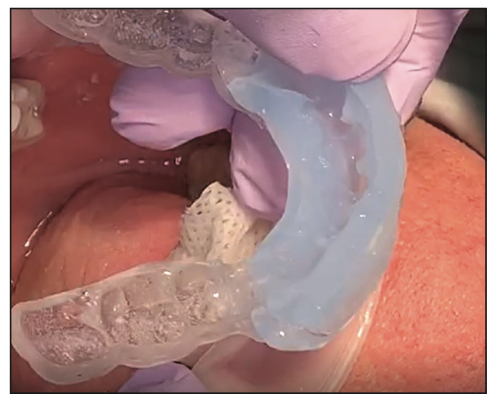
Figure 13. Clear PVS made off the wax-up and accurately transfering the composite to the mouth.
Accurate PVS impressions were taken, and models were poured and mounted on an AD2 semi-adjustable articulator utilizing the AD2 Easy Bow transfer. The diagnostic wax-up (Figure 12) was completed by the author. Clear stints were made to transfer the wax-up morphology to the mouth in composite (Figure 13).
Restorative Treatment
The anterior teeth were restored first (Figure 14). The teeth were conservatively prepped for composite veneers and then restored utilizing the clear stints. Centric contacts were established (Figure 15) with little adjustments as the stints provided a fully accurate transfer of the composite to the mouth. Next, the maxillary and mandibular posterior teeth were restored. The zirconia crowns on teeth Nos. 3, 14, and 19 were replaced with lithium disilicate crowns.

Figure 14. Anterior teeth restored with composite.

Figure 15. Centric contact on lower anterior teeth.
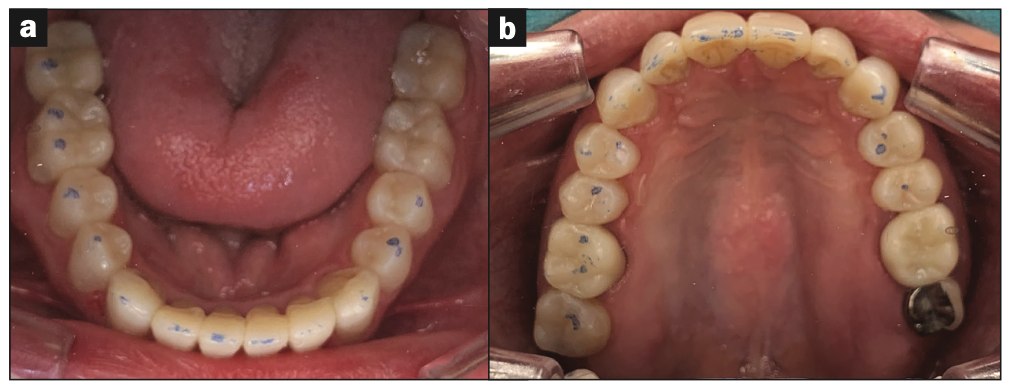
Figure 16. (a) All mandibular teeth restored and showing stable centric contacts. (b) All maxillary teeth restored and showing stable centric contacts.
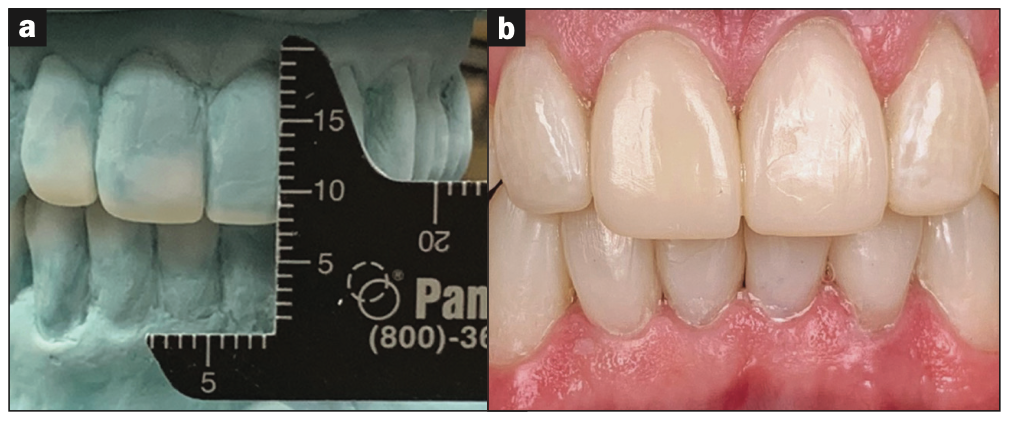
Figure 17. (a) Improved VDO as measured on the wax-up and (b) in the mouth.
The occlusion was verified, and minor adjustments were made (Figure 16). The VDO was verified and compared to the wax-up (Figure 17).
Final Restorative Outcome
The patient was successfully restored post-orthodontically with an increased VDO, a fully functional anterior proprioceptive occlusion, and an optimal smile and facial aesthetics. It is important to note the overall improvements in the patient’s facial features (Figure 18) and muscle tone because of the harmony created in the stomatognathic system. The optimized occlusal scheme requires little pressure from the teeth as a result of the verticalized biological anatomy and muscle harmony.
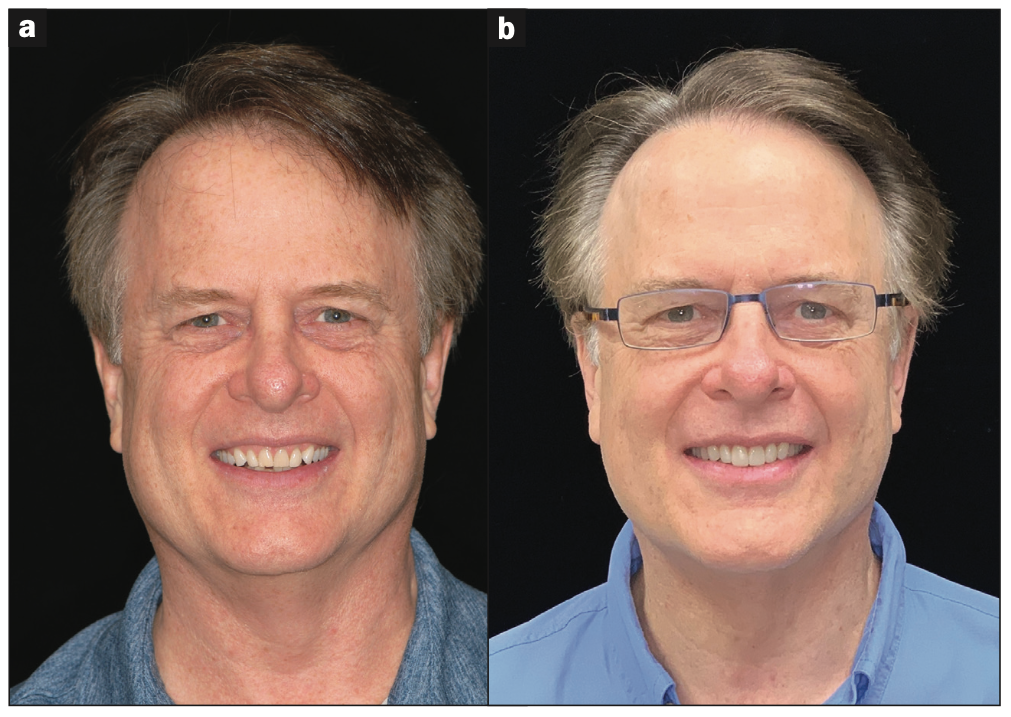
Figure 18. (a) Pre-op photo and (b) post-op photo. Note relaxed muscles and improved facial aesthetics.
L.D. Pankey’s rules of optimal occlusion state the following:
l With the condyles fully seated in the fossa, all the posterior teeth occlude simultaneously and evenly, with the anterior lightly touching.
l When the patient squeezes, neither a tooth nor the mandible moves.
l When the mandible is moved in any excursion, no back teeth touch before, harder than, or after a front tooth.
All these rules were met in this case.
Airway Improvement
The previously mentioned 3.0-mm transverse width increase in both dental arches, along with the increased VDO, resulted in an increase of the functional airway (Figure 19). The minimally restricted area went from a preoperative measurement of 206 mm2 to a postoperative measurement of 240 mm2. The total volume went from a pre-op volume of 13 cm3 to a post-op volume of 24 cm3. This exponential increase in total volume is consistent with Poiseuille’s Law, which shows an exponential increase in volume through a tube or cylinder when the surface area increases. In this case, the surface area of the minimally restricted area was increased by 14%, yet the air volume increased by 46%. It does not take a huge increase in surface area to create a significant increase in volume. This had a positive effect on the patient, who stated that he no longer snores, no longer clenches his teeth, and feels better overall. The increase in arch space allowed the mandible to move into a more favorable condylar position, as the post-op image shows the condyles are no longer distally positioned (Figure 20).
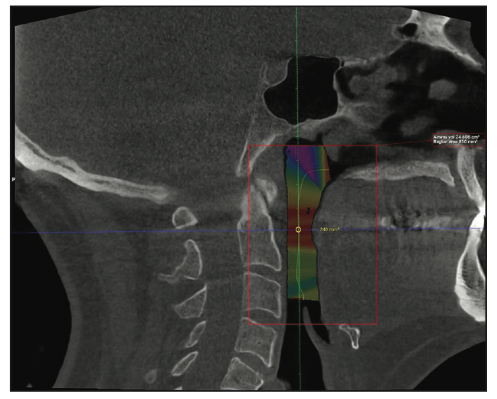
Figure 19. Post-op CBCT. The minimally restricted area was increased 14% (from 206 mm2 to 240 mm2) and this resulted in a 46% increase in total airway volume (from 13 cm3 to 24 cm3).
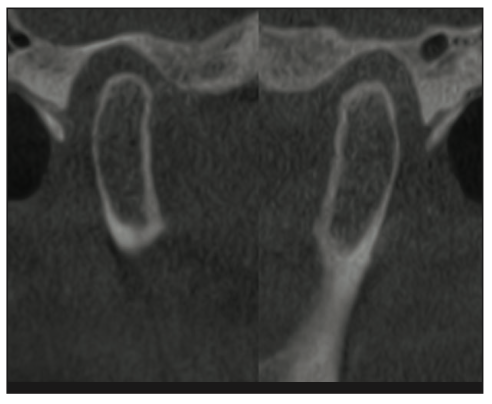
Figure 20. Post-op condyles are in a more favorable anterior position.
This condylar position was then stabilized with accurate, stable centric contact points as previously shown.
CONCLUSION
An aesthetic and functional result was achieved by addressing the patient’s oral needs with an airway-positive approach, thus creating more tongue and functional airway space prior to restoration. Tried and true occlusion principles were then applied utilizing minimally invasive additive techniques, or as the author calls it, the bio-rejuvenation technique. The patient is breathing and sleeping better. He is comfortable and happy with the final aesthetic outcome.
The author has been practicing bio-rejuvenation dentistry since 2001. He has added the airway occlusion approach over the past 10 years and has restored hundreds of patients in this manner. While each case is different, the results are consistent if the principles of adequate airway space, stable TMJs, interarch relationship, and biologic tooth morphology are met.
REFERENCES
1. Thuler E, Rabelo FAW, Yui M, et al. Correlation between the transverse dimension of the maxilla, upper airway obstructive site, and OSA severity. J Clin Sleep Med. 2021;17(7):1465–73. doi:10.5664/jcsm.9226
2. Lee RL. Esthetics and its relationship to function. In: Refenacht CR, ed. Fundamentals of Esthetics. Quintessence Publishing; 1990:137-208.
3. Simmons J, Prehn P. The missing link between nocturnal bruxism and obstructive sleep apnea. Poster presented at: SLEEP 2008: 22nd Annual Meeting of the Associated Professional Sleep Societies; June, 2008; Baltimore, MD.
4. Sharma K, Shrivastav S, Hotwani K. Volumetric MRI evaluation of airway, tongue, and mandible in different skeletal patterns: does a link to obstructive sleep apnea exist (OSA)? Int J Orthod Milwaukee. 2016;27(3):39-48.
5. Jena AK, Singh SP, Utreja AK. Sagittal mandibular development effects on the dimensions of the awake pharyngeal airway passage. Angle Orthod. 2010;80(6):1061–7. doi:10.2319/030210-125.1
6. Stewart H. Conservative Full Mouth Rehabilitation Using The Principles of Bioesthetic Dentistry. Contemporary Esthetics. 2006;10:46-56
ABOUT THE AUTHOR
Dr. Stewart has been practicing dentistry in Flower Mound, Texas, since 1990. He is co-founder and CEO of the Stewart Center for Minimally Invasive Dental Medicine. He is also on the teaching faculty of the Breathe Institute in Los Angeles, Calif. Dr. Stewart can be reached at drhal@thestewartcenter.com.
Disclosure: The author reports no disclosures.