
Teeth selection
The protocol of this study was approved by an institutional review board from King Abdullah International Medical Research Center (RC20/570/R). All methods were performed in compliance with the relevant guidelines and regulations.
Intact permanent premolar teeth with single canals were selected and stored in distilled water. The teeth were extracted for unknown reasons after obtaining informed consent from patients. They were inspected under a dental operating microscope at 4 × magnification (OPMI Zeiss Pico; Carl Zeiss MediTec, Dublin, CA, USA) to detect root surface defects. They were radiographically observed in buccolingual and mesiodistal aspects. Teeth with oval straight canals were included if the canal diameter in the buccolingual aspect was at least twice larger than the mesiodistal diameter at any level in the coronal two-thirds of the canal. Teeth with curved canals, incomplete roots, root cracks, wide apex, or root canal filling were excluded.
Based on a pilot study and using a two-sample t-test, the sample size was calculated (PiFace, http://homepage.stat.uiowa.edu/~rlenth/Power/) with an 80% power and 5% significance level. The minimum mean differences (standard deviations) of the retreatment time, maximum load, maximum torque, and remaining obturating materials percentage were set found to be 9 (6), 0.5 (0.4), 0.4 (0.3), and 7 (5), respectively. According to these parameters, a minimum number of eleven samples per each group was required.
Sample preparation
The tooth root was covered with aluminum foil which was then immersed in a mixed resin (Duralay; Reliance Dental Mfg, Worth, IL, USA) inside a 12-mm height plastic transparent tube. After the resin set, the foil was removed and a light-body silicone impression material was added to simulate the periodontal ligament. Access cavity was created and a size 10 K-file file (SybronEndo, Orange, CA, USA) was used to verify canal patency and set the working length short of the foramen by 0.5 mm. The manual glide path was made up to size 15 K-file. Then, canals were prepared with HyFlex CM rotary file (Coltène Whaledent, Altstätten, Switzerland) to size 30, 0.04. Canal patency was maintained through recapitulation and irrigation with 5 ml of 2.5% sodium hypochlorite (NaOCl) throughout the canal preparation. Finally, the canals were irrigated with 2 ml of 17% EDTA and flushed with 2 ml of 0.9% sodium chloride. A 27G side-vented irrigating needle was used during the irrigation step.
The prepared canals were coded and distributed randomly (using www.random.org) into two groups of 12 samples based on the endodontic sealer used: AHP and TFBC.
Canal obturation
Each canal was obturated with a matched gutta-percha cone size 30, 0.04 according to manufacturers’ instructions. The canals were dried completely with matching paper points.
For the AHP group, the sealer was placed with a sterilized K-file. Also, the cone was coated with the sealer and inserted to the working length. For the TFBC group, the sealer was injected after positioning the syringe tip in the root canal. Then, the cone was coated with TFBC and inserted to the working length.
The excess gutta-percha was cut using B&L SuperEndo Alpha II unit (B&L BioTech, Philadelphia, PA, USA) at a level below the orifice. Then, the samples were coronally temporized with Coltosol F (Coltène Whaledent, Altstätten, Switzerland), and periapical radiographs were obtained to check the quality of the obturation. In case of unsatisfactory obturation quality, the sample was discarded and replaced. Then, the samples were placed in a test tube containing phosphate-buffered saline (PBS) and incubated for 6 months at 37 °C and 100% humidity. Canal shaping and obturation were performed by a single operator (Az. A).
Micro-computed tomography (micro-CT) examination
Each sample was scanned twice (before and after the retreatment procedure) using a micro-CT device (SkyScan 1172; Bruker micro-CT, Kontich, Belgium) with the following parameters: 70 kV, 139 μA, aluminum filter with 0.5 mm thickness, voxel size of 13.6 μm, rotational step of 0.80-degree, rotational angle of 180-degree, exposure time of 2 s, and 3X frame averaging.
The resultant JPG slices were used to create 3D reconstruction using NRecon software (Bruker micro-CT) with 10X ring artifact correction and 50% beam hardening correction.
CTAn software (Bruker micro-CT) was used to perform segmentation and thresholding for the apical 12 mm of the sample to measure the volumes of obturating materials before and after retreatment. The percentage of the remaining obturating material was calculated by dividing the volume of the remaining obturating material after retreatment by the volume of the obturating material before retreatment and multiplying the result by 100.
Canal retreatment
The coronal 2 mm of obturating materials were removed using a size 3 Gates Glidden drill (Dentsply Sirona, Ballaigues, Switzerland). Then, 1–2 drops of chloroform were used to soften the obturating material to facilitate file penetration. WOG Primary file (size 25, 0.07) was operated with reciprocating motion using the “WAVEONE ALL” mode in the X-Smart Plus motor (Dentsply Sirona) to remove the obturating materials. Attempts were made to reach the working length. Then, 10 vertical brushing movements with 3 mm amplitude were performed. Afterward, the canal was dried with paper points and checked for remnants of gutta-percha under the microscope at 8 × magnification. When gutta-percha was found on the canal walls, another 10 vertical strokes were performed. The canals were irrigated using a 27G side-vented irrigating needle with a total of 9 ml volume (5 ml of 2.5% NaOCl throughout the procedure and a final rinse of 2 ml of 17% EDTA was performed before flushing with 2 ml of 0.9% sodium chloride). The total amount of time needed for retreatment by the use of the WOG Primary file inside the canal, including the additional strokes, where applicable, and irrigation was calculated. Regaining the apical patency was inspected using a size 15 K-file.
To mimic the clinical conditions, the procedure was conducted while the sample was surrounded with warm water at 35 ± 1 °C.
Load and torque measurements
A load gauge (M5-20 Advanced Digital Force Gauge; Mark- 10 Corporation) and a torque gauge (TT01 torque Gauge; Mark-10 Corporation) were used in the current study and were checked for accuracy before the retreatment. The load gauge was centered and fixed in a standing position above the torque gauge. Then, each sample was secured at the top of the load gauge. With this, measuring the developed real-time vertical load and torque simultaneously using MESUR Lite software (Mark-10 Corporation, Copiague, NY, USA) was possible (Fig. 1). The apically directed load represents the positive load required to advance the file inside the canal. The coronally directed load represents the load required to remove the file from the canal against resistance. The positive torque values were observed. The gauge devices measured data every 0.1 s.
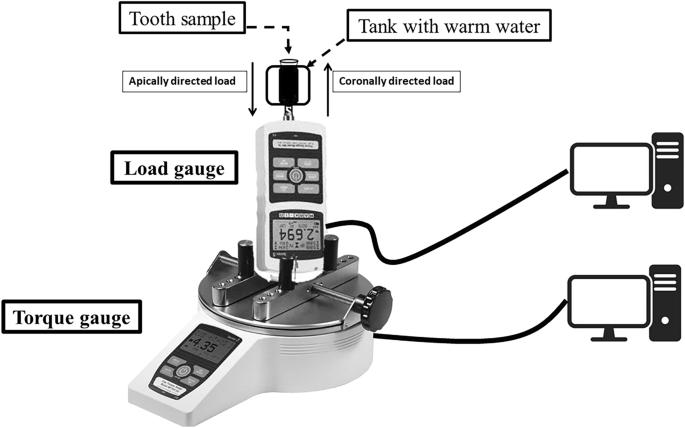
Schematic drawing of the experimental set-up.
Statistical analysis
Statistical analyses were performed using the statistical program SPSS version 22 (IBM, Chicago, IL, USA) at a 95% confidence level. Since the distribution of the tested variables data was normal by the Kolmogorov–Smirnov test (P > 0.05), the independent t-test test was used to compare the experimental groups in terms of the effective retreatment time, the maximum load in apical and coronal directions, the maximum torque, and the percentage of remaining obturating materials. The number of teeth where apical patency was regained in both groups was compared by employing the chi-square test.